

Mutational Profile in 75 Patients With Anti-Myelin-Associated Glycoprotein Neuropathy: Clinical and Hematologic Therapy Response and Hints on New Therapeutic Targets
- PMID: 37137530
- PMCID: PMC10155778
- DOI: 10.1212/NXI.0000000000200122
Mutational Profile in 75 Patients With Anti-Myelin-Associated Glycoprotein Neuropathy: Clinical and Hematologic Therapy Response and Hints on New Therapeutic Targets
Abstract
Background and objectives: Neuropathy with antibodies to myelin-associated glycoprotein (MAG) is the most common paraproteinemic IgM neuropathy. Recently, the mutational profile of the MYD88 and CXCR4 genes has been included in the diagnostic workup of IgM monoclonal gammopathies. The objective of our study was to assess the prevalence of MYD88 L265P and CXCR4 S338X gene variants in patients with anti-MAG antibody neuropathy. Secondary aims were to evaluate possible correlations between the mutational profile and neuropathy severity, antibody titers, and treatment response.
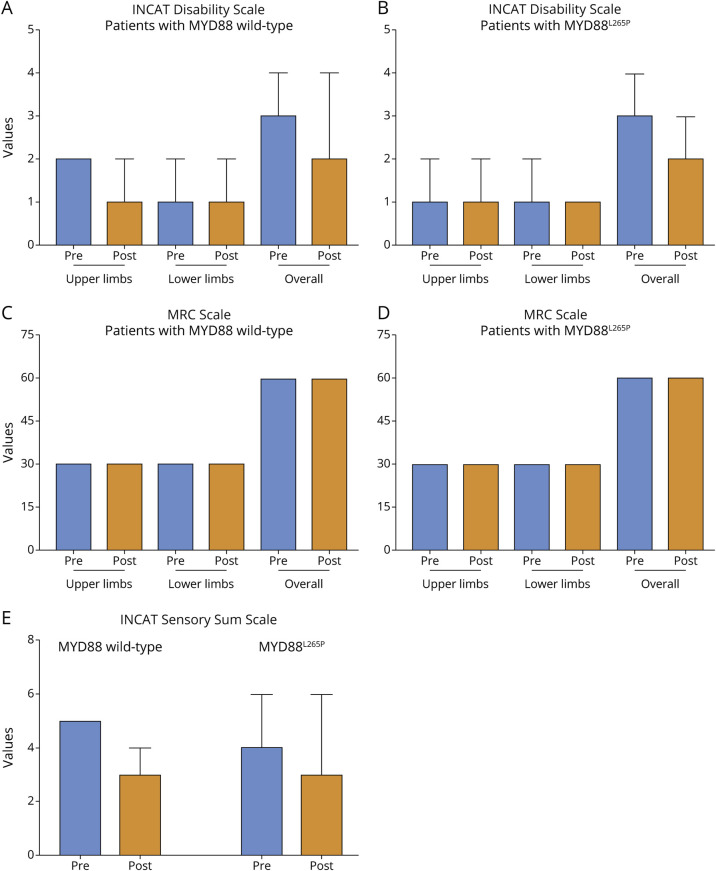
Methods: Seventy-five patients (47 men, mean age at molecular analysis 70.8 ± 10.2 years; mean disease duration 5.1 ± 4.9 years) with anti-MAG antibody neuropathy were recruited. Among them, 38 (50.7%) had IgM monoclonal gammopathy of undetermined significance, 29 (38.7%) Waldenstrom macroglobulinemia (WM), and 8 (10.6%) chronic lymphocytic leukemia/marginal zone lymphoma/hairy cell leukemia variant. Molecular analysis was performed on DNA from the bone marrow mononuclear cells in 55 of 75 patients and from peripheral mononuclear cells in 18 of 75 patients. Forty-five patients were treated with rituximab, 6 with ibrutinib, 2 with obinutuzumab-chlorambucil, and 3 with venetoclax-based therapy. All the patients were assessed with the Inflammatory Neuropathy Cause and Treatment (INCAT) Disability Scale, INCAT Sensory Sum Score, and MRC Sum Score at baseline and follow-up. We considered as responders, patients who improved by at least 1 point in 2 clinical scales.
Results: Fifty patients (66.7%) carried the MYD88L265P variant, with a higher frequency in WM and naive patients (77.2% vs 33.3%, p = 0.0012). No patients harbored the CXCR4S338X variant. There were no significant differences in hematologic data (IgM levels, M protein, and anti-MAG antibody titers), neuropathy severity, or response to rituximab in MYD88-altered and MYD88 wild-type patients. Nine of 11 (81.8%) patients treated with novel targeted drug, according to the MYD88 status, responded to treatments.
Discussion: MYD88L265P variant has a high prevalence (66.7%) in anti-MAG antibody neuropathy representing a potential effective mutational target for Bruton tyrosine kinase inhibitors. MYD88L265P variant, however, does not seem to be a prognostic factor of neuropathy severity or response to rituximab. In patients not responding or becoming refractory to rituximab, a tailored therapy with new effective target therapies should be considered.
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Academy of Neurology.
Conflict of interest statement
F. Castellani reports no disclosures; A. Visentin is in the advisory board of Janssen and BeiGene; E. Schirinzi, A. Salvalaggio, M. Cacciavillani, C. Candiotto, C. Baratè, A. Cellini, R. Bertorelle, and G. Siciliano report no disclosures; L. Trentin is in the advisory board of Janssen and BeiGene; C. Briani reports no disclosures. Go to
Figures
References
-
- Parisi M, Dogliotti I, Clerico M, et al. Efficacy of rituximab in anti-myelin-associated glycoprotein demyelinating polyneuropathy: clinical, hematological and neurophysiological correlations during 2 years of follow-up. Eur J Neurol. 2022;29(12):3611-3622. doi. 10.1111/ene.15553 - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials