

The hydrocortisone-responsive urinary metabolome of premature infants
- PMID: 37138028
- PMCID: PMC10589081
- DOI: 10.1038/s41390-023-02610-5
The hydrocortisone-responsive urinary metabolome of premature infants
Abstract
Background: Extremely premature infants are at risk for circulatory collapse or respiratory failure that are often treated with hydrocortisone (HC); however, there is no information on the metabolic consequences of this therapy.
Methods: Longitudinal urine samples from infants <28 weeks gestation in the Trial of Late Surfactant were analyzed by untargeted UHPLC:MS/MS. Fourteen infants who received a tapering course of HC beginning at 3 mg/kg/day for ≥9 days were compared to 14 matched control infants. A secondary cross-sectional analysis by logistic regression used urines from 314 infants.
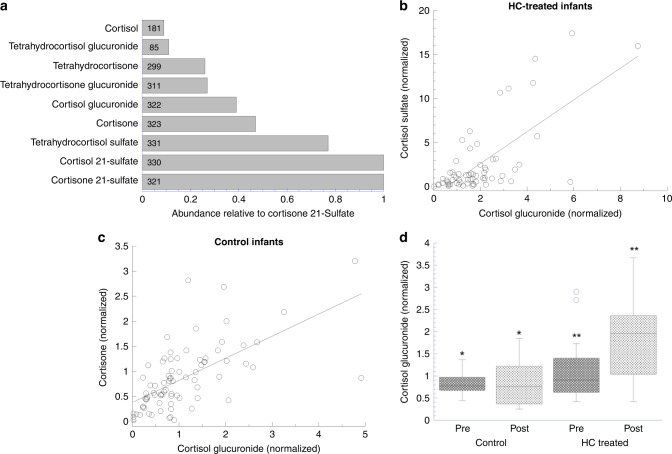
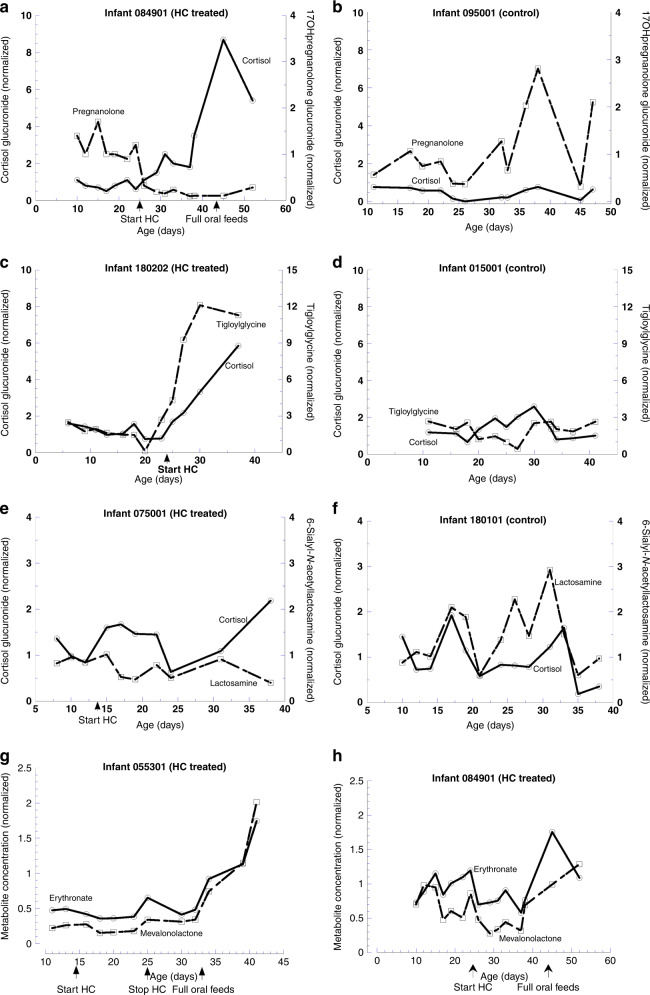
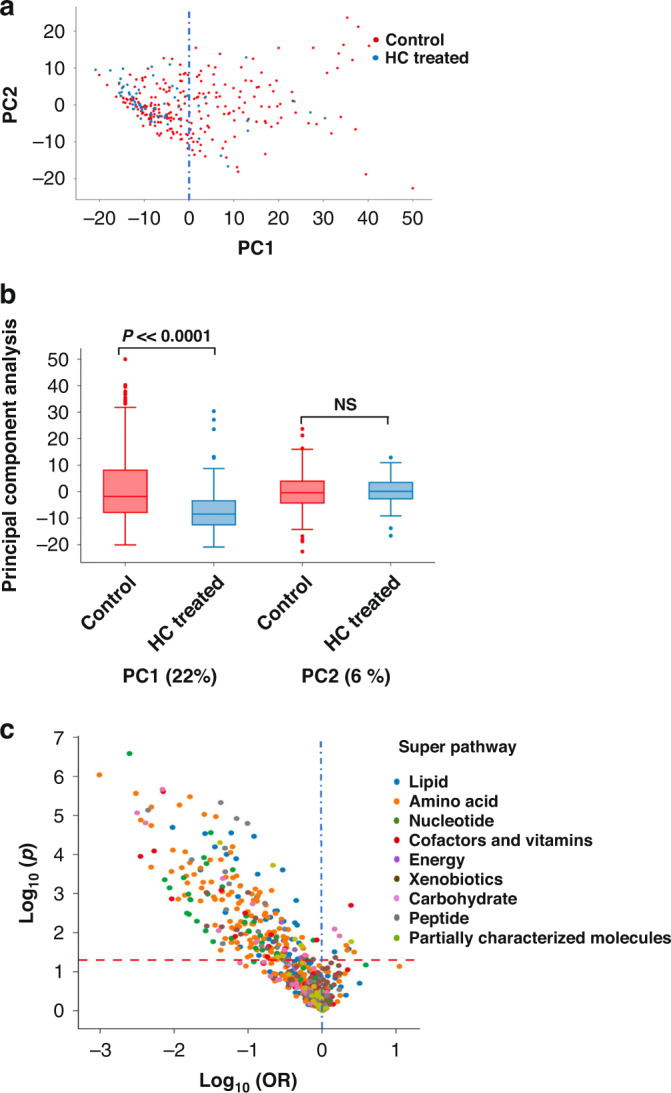
Results: Of 1145 urinary metabolites detected, abundance of 219, representing all the major biochemical pathways, changed at p < 0.05 in the HC-treated group with 90% decreasing; 3 cortisol derivatives increased ~2-fold with HC therapy. Only 11% of regulated metabolites remained responsive at the lowest HC dose. Regulated metabolites included two steroids and thiamin that are associated with lung inflammation in infants. HC responsiveness was confirmed in 57% of metabolites by cross-sectional analysis.
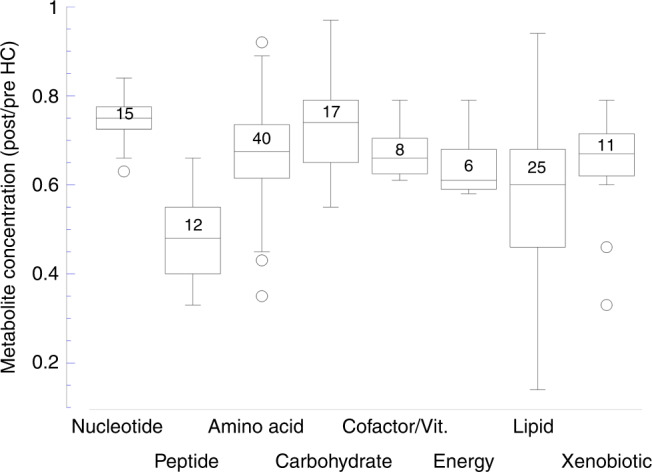
Conclusions: HC treatment of premature infants influenced in a dose-dependent manner abundance of 19% of identified urinary metabolites of diverse biochemical systems, primarily reducing concentrations. These findings indicate that exposure to HC reversibly impacts the nutritional status of premature infants.
Impact: Hydrocortisone treatment of premature infants with respiratory failure or circulatory collapse alters levels of a subset of urinary metabolites representing all major biochemical pathways. This is the first description of the scope, magnitude, timing and reversibility of metabolomic changes in infants in response to hydrocortisone, and it confirms corticosteroid regulation of three biochemicals that are associated with lung inflammatory status. The findings indicate a dose-dependency of hydrocortisone for metabolomic and anti-inflammatory effects, that prolonged therapy may lower the supply of many nutrients, and that monitoring concentrations of cortisol and inflammation markers may be a useful clinical approach during corticosteroid therapy.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Mesiano S, Jaffe RB. Developmental and functional biology of the primate fetal adrenal cortex. Endocr. Rev. 1997;18:378–403. - PubMed
