

High prevalence of sacroiliitis and early structural changes in the sacroiliac joint in children with enthesitis-related arthritis: findings from a tertiary centre in Hong Kong
- PMID: 37138335
- PMCID: PMC10158136
- DOI: 10.1186/s12969-023-00825-8
High prevalence of sacroiliitis and early structural changes in the sacroiliac joint in children with enthesitis-related arthritis: findings from a tertiary centre in Hong Kong
Abstract
Background: Epidemiological studies have demonstrated a wide, unexplained disparity in the prevalence of juvenile idiopathic arthritis (JIA) subtypes depending on geographical location, ethnicity and other factors. Enthesitis-related arthritis (ERA) is more prevalent in Southeast Asia. Axial involvement in ERA patients is increasingly recognised to occur early in the disease course. Inflammation in the sacroiliac joint (SIJ) observed on MRI seems highly predictive of subsequent structural radiographic progression. The resulting structural damage can have significant impacts on both functional status and spinal mobility. This study aimed to evaluate the clinical characteristics of ERA in a tertiary centre in Hong Kong. The primary objective of the study was to provide a comprehensive description of the clinical course and radiological findings of the SIJ among ERA patients.
Method: Paediatric patients diagnosed with JIA attending the paediatric rheumatology clinic from January 1990 to December 2020 were recruited from our registry based at the Prince of Wales Hospital.
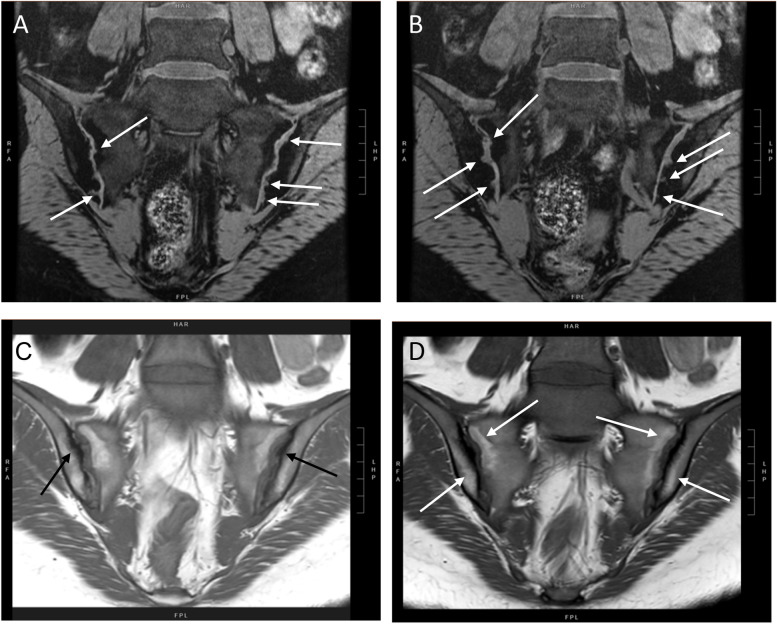
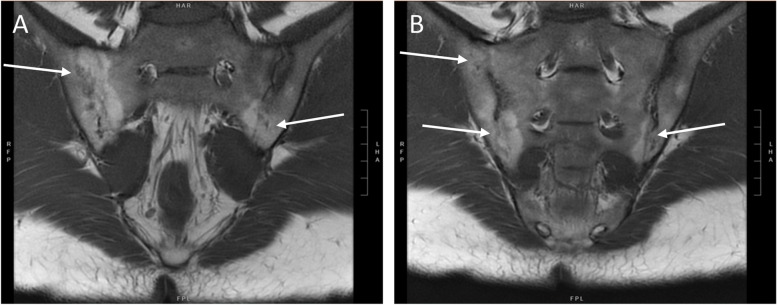
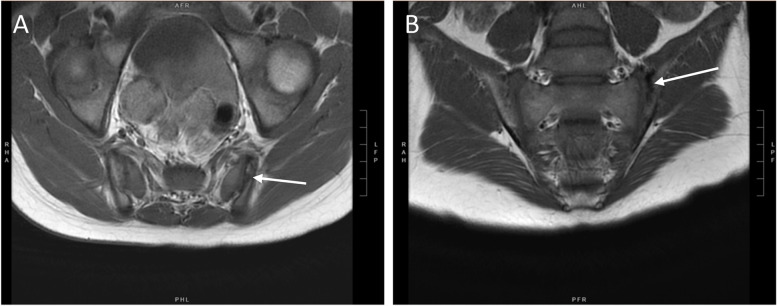
Results: In our cohort, 101 children were included. The median age of diagnosis was 11 years, interquartile range (IQR) 8-15 years. The median follow-up duration was 7 years (IQR 2-11.5 years). ERA was the most prevalent subtype (40%), followed by oligoarticular JIA (17%). Axial involvement was frequently reported in our cohort of ERA patients. 78% demonstrated radiological evidence of sacroiliitis. Among those, 81% had bilateral involvement. The median duration from disease onset to confirmation of radiological sacroiliitis was 17 months (IQR 4-62 months). Among the ERA patients, 73% had structural changes of the SIJ. Alarmingly, 70% of these patients had already developed radiological structural changes when sacroiliitis was first detected on imaging (IQR 0-12 months). Erosion was the most common finding (73%), followed by sclerosis (63%), joint space narrowing (23%), ankylosis (7%) and fatty change (3%). The duration from symptom onset to diagnosis was significantly longer in ERA patients with SIJ structural changes (9 vs 2 months, p = 0.009), comparing with those without.
Conclusion: We found that a high proportion of ERA patients had sacroiliitis and a significant number of them had radiological structural changes during early disease. Our findings illustrate the importance of prompt diagnosis and early treatment in these children.
Keywords: Enthesitis-related arthritis; Juvenile idiopathic arthritis; Sacroiliac joint; Sacroiliitis.
© 2023. The Author(s).
Conflict of interest statement
All authors declared no conflict of interest in relation to this study.
Figures
References
-
- Petty RE, Southwood TR, Manners P, Baum J, Glass DN, Goldenberg J, et al. International League of Associations for Rheumatology classification of juvenile idiopathic arthritis: second revision, Edmonton, 2001. J Rheumatol. 2004;31(2):390–392. - PubMed
-
- Consolaro A, Giancane G, Alongi A, van Dijkhuizen EHP, Aggarwal A, Al-Mayouf SM, et al. Phenotypic variability and disparities in treatment and outcomes of childhood arthritis throughout the world: an observational cohort study. Lancet Child Adolesc Health. 2019;3(4):255–263. doi: 10.1016/S2352-4642(19)30027-6. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
