

doi: 10.1016/j.eats.2022.11.030.
eCollection 2023 Apr.
Open Latarjet with Metal-Free Cerclage Fixation
Affiliations
- PMID: 37138684
- PMCID: PMC10149785
- DOI: 10.1016/j.eats.2022.11.030
Item in Clipboard
Open Latarjet with Metal-Free Cerclage Fixation
Arthrosc Tech.
.
Abstract
Despite multiple modifications, the Latarjet is still the most popular procedure for recurrent anterior shoulder instability with glenoid bone loss. Partial or subtotal resorption of the graft is common, potentially leading to hardware prominence and risk of anterior soft-tissue impingement. To minimize the technical difficulties and morbidity associated with metallic implants, a coracoid and conjoint tendon transfer with a mini-open approach using Cerclage tape suture is described, as an alternative for the Latarjet procedure typically performed with metal screws and plates.
© 2022 The Authors.
Figures
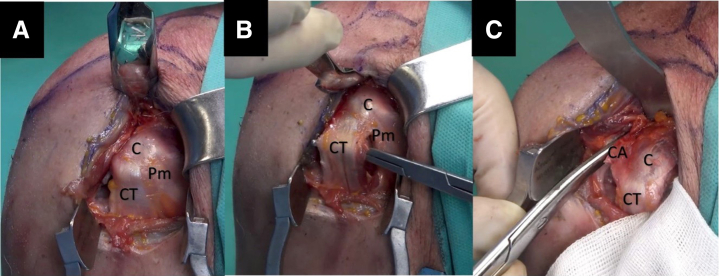
Right shoulder, beach-chair position, anterior view. (A-C) A 5-cm vertical incision is made, from the tip of the coracoid process to the axilla. The deltopectoral grove is opened. The coracoacromial ligament must be released laterally, leaving a small stump and the pectoralis minor medially. The conjoined tendon should be isolated and protected. (C, coracoid process; CA, coracoacromial ligament; CT, conjoined tendon; Pm, pectoralis minor.)

Right shoulder, beach-chair position, anterior view. (A) Using an angle motorized saw, perform the osteotomy of the coracoid process at its base. (B) With skin, the marker identifies and draws 2 points separated by 1 cm in the coracoid graft. (C) While securing the graft, drill two 3-mm holes following the previous marks on the graft (arrowheads). (D) secure the coracoid using a suture around its base during the surgery (arrow).

Right shoulder, beach-chair position, posterosuperior view. (A) Introduce a Wissinger rod through the anterior incision, across, and parallel to the glenohumeral joint. Mark the point where the rod pushes the posterior skin. Make a horizontal incision (black star) at that level and pass the Wissinger rod. (B-D) The half-pipe cannula should be introduced following the switching stick from anterior to posterior. Once the cannula is through, the hook guide is inserted from posterior to anterior over the half pipe. The hook is then centered on the glenoid rim defect. (E-F) A specific sleeve drill guide (Arthrex) is assembled to the handle of the hook and introduced using the posterior incision. (B, anterior aspect of the shoulder; G, hook guide; HC, half-pipe cannula; SG, specific sleeve drill guide; W, Wissinger rod.)

Right shoulder, beach-chair position, anterior view. (A) Split through the subscapularis tendon between the middle and inferior third, with the arm in adduction and external rotation to tension the muscle. (B-C) While feeling the joint line, a vertical incision is made to the capsule medially, leaving a stump for the posterior repair. Using the small glenoid retractor medially and a Fukuda retractor, the anterior surface of the glenoid neck should be debrided to enhance graft healing. Arrow: Suture attached to the coracoid process base. (A, anterior glenoid neck; JL, joint line; SSC, subscapularis tendon.)

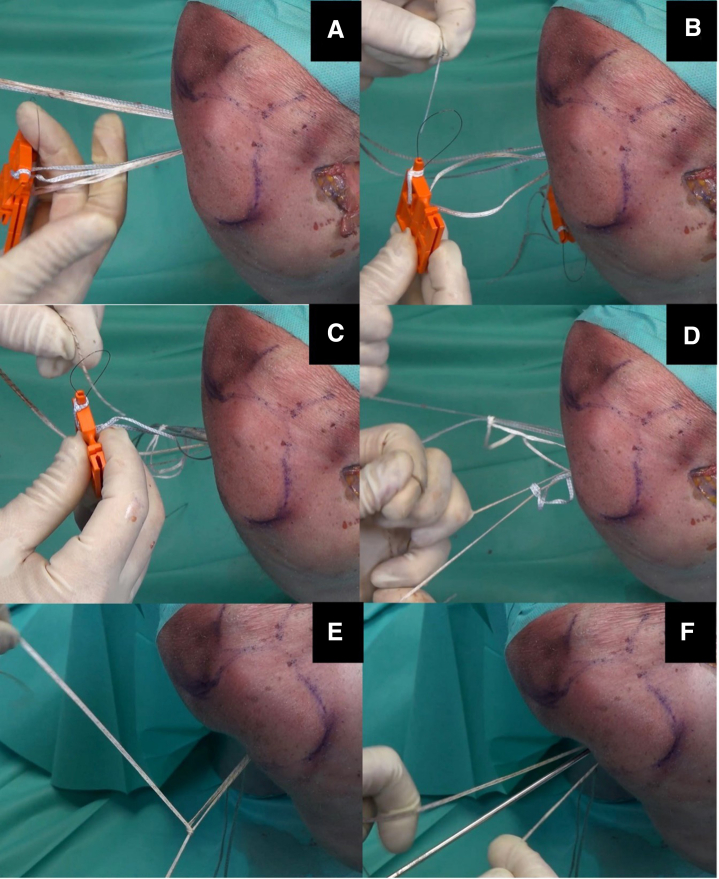
Right shoulder, beach-chair position, anterior view. (A) A 3-mm cannulated drill is passed through both sleeve guide holes until exiting on the anterior aspect of the glenoid. Pass 2 nitinol wires through the cannulated drill (arrows). (B) Replace the nitinol wires with 2 different colors of high-strength sutures link (Arthrex) to avoid breakage during traction. (C-F) Introduce and secure 2 preconfigured cerclage suture tapes (Arthrex) with the same length and tension to the one suture Link with the loop posteriorly. Get them through the respective tunnel in the graft (arrowhead) and floss them. Finally retrieve them through the second tunnel in the graft, forming a U cerclage, and retrieve them through the second suture link with the anterior loop. (A, anterior surface of the glenoid; C, coracoid process; F, high-strength FiberLink; JL, joint line; NW, nitinol wire; T, cerclage tapes.)
Right shoulder, beach-chair position superior view. (A-B) Once the cerclage tapes are recovered on the posterior aspect of the shoulder, we interconnect the tapes using the nitinol loop of the preconfigured knot, completing the cerclage suture system. (C-D) Pulling from each suture limb of both cerclages alternatively and symmetrically the knots slide against the posterior glenoid neck. (E-F) Lock the system with alternate four-half hitch knots using the knot-pusher while holding the post aside.
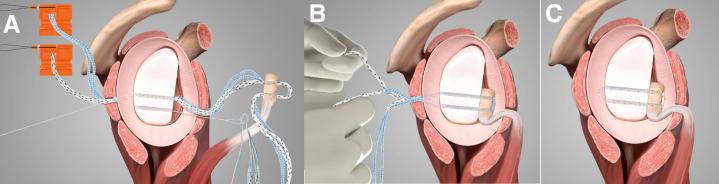
Right shoulder, sagittal view, the final scheme. (A-C) Two cerclage suture tapes (Arthrex) are passed through the proximal glenoid tunnel and through the coracoid graft. Using a high-strength suture link (Arthrex) the suture tapes are retrieved to the posterior aspect of the glenoid neck. (B) Once the cerclage suture system is interconnected, each suture limb is pulled alternatively and symmetrically sliding the knots against the posterior glenoid neck. (C) Final view of the construct locked with four-half hitch knots and knot-pusher.
References
-
- Balg F., Boileau P. The instability severity index score. A simple pre-operative score to select patients for arthroscopic or open shoulder stabilisation. J Bone Joint Surg Br. 2007;89:1470–1477. - PubMed
-
- Boileau P., Villalba M., Héry J.Y., Balg F., Ahrens P., Neyton L. Risk factors for recurrence of shoulder instability after arthroscopic Bankart repair. J Bone Joint Surg Am. 2006;88:1755–1763. - PubMed
-
- Gouveia K., Abidi S.K., Shamshoon S., et al. Arthroscopic Bankart Repair with remplissage in comparison to bone block augmentation for anterior shoulder instability with bipolar bone loss: A systematic review. Arthroscopy. 2021;37:706–717. - PubMed
-
- Hurley ET, Montgomery C, Jamal MS, et al. Return to play after the Latarjet procedure for anterior shoulder instability: A systematic review [published correction appears in Am J Sports Med 2019;47:NP48]. Am J Sports Med 2019;47:3002-3008. - PubMed
-
- Hurley E.T., Lim Fat D., Farrington S.K., Mullett H. Open versus arthroscopic Latarjet procedure for anterior shoulder instability: A systematic review and meta-analysis. Am J Sports Med. 2019;47:1248–1253. - PubMed
