

FLAIR-hyperintense lesions in anti-MOG-associated encephalitis with seizures overlaying anti-N-methyl-D-aspartate receptor encephalitis: a case report and literature review
- PMID: 37138864
- PMCID: PMC10150000
- DOI: 10.3389/fimmu.2023.1149987
FLAIR-hyperintense lesions in anti-MOG-associated encephalitis with seizures overlaying anti-N-methyl-D-aspartate receptor encephalitis: a case report and literature review
Abstract
Background: FLAIR-hyperintense lesions in anti-MOG-associated encephalitis with seizures (FLAMES) has been identified increasingly frequently in recent years. However, this rare MOG antibody disease may coexist with anti-N-methyl-D-aspartate receptor encephalitis (anti-NMDARe), in an overlap syndrome with unknown clinical features and prognosis.
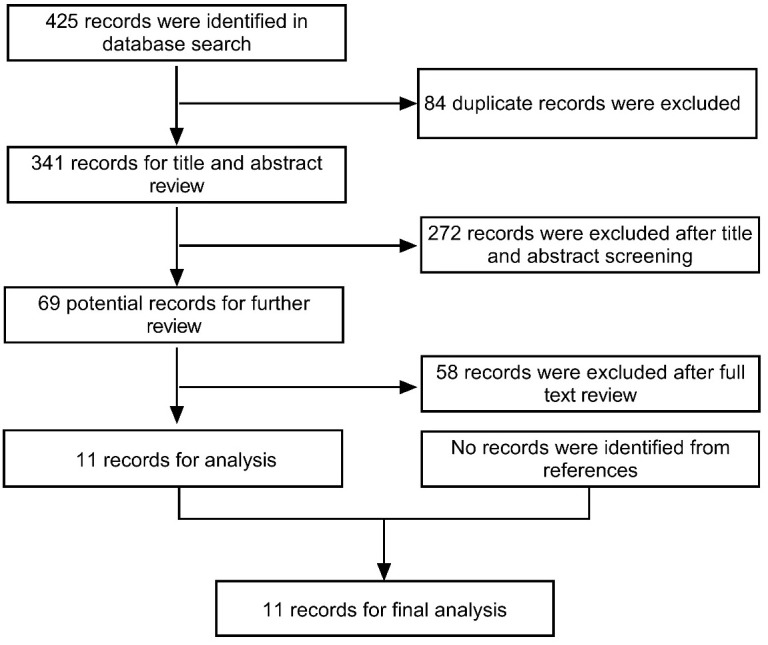
Methods: We report a new case of this overlap syndrome and present a systematic review of similar cases in the literature to provide information on the clinical presentation, MRI features, EGG abnormalities, treatment, and prognosis of patients with this rare syndrome.
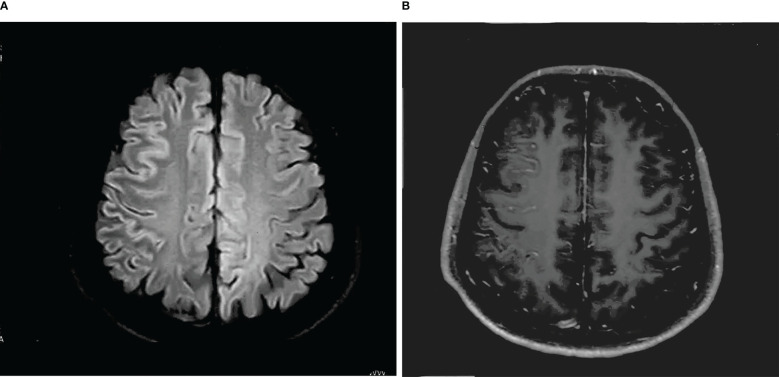
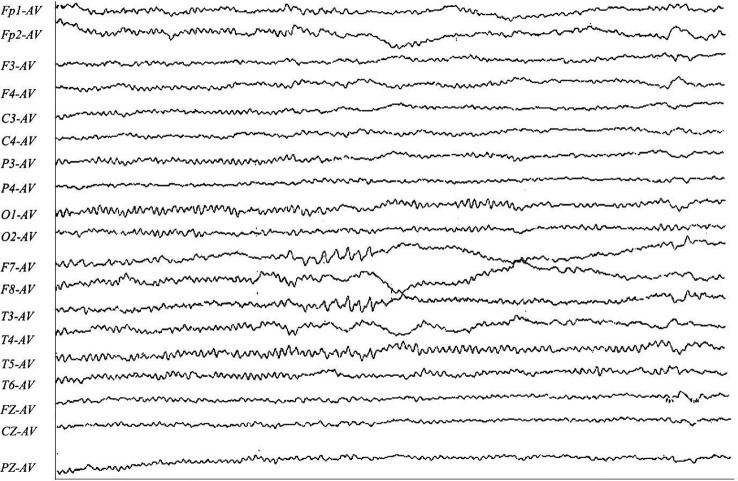
Results: A total of 12 patients were analyzed in the study. The most common clinical manifestations of FLAMES overlaid with anti-NMDARe were epilepsy (12/12), headache (11/12), and fever (10/12). Increases in intracranial pressure (median: 262.5 mmH2O, range: 150-380 mmH2O), cerebrospinal fluid (CSF) leukocyte count (median: 128×106/L, range: 1-610×106/L), and protein level (median: 0.48 g/L) were also observed. The median CSF anti-NMDAR antibody titer was 1:10 (1:1-1:32), while the median serum MOG antibody titer was 1:32 (1:10-1:1024). Seven cases exhibited unilateral cortical FLAIR hyperintensity, and five cases (42%) had bilateral cortical FLAIR hyperintensity, including four cases involving the bilateral medial frontal lobes. Of the 12 patients, five showed lesions at other sites (e.g., the brainstem, corpus callosum, or frontal orbital gyrus) before or after the development of cortical encephalitis. EEG showed slow waves in four cases, spike-slow waves in two cases, an epileptiform pattern in one case, and normal waves in two cases. The median number of relapses was two. Over a mean follow-up period of 18.5 months, only one patient experienced residual visual impairment, while the remaining 11 patients had good prognoses.
Conclusion: FLAMES alone is difficult to distinguish from overlap syndrome based on clinical features. However, FLAMES with bilateral medial frontal lobe involvement suggests the presence of the overlap syndrome.
Keywords: FLAIR; MOG ab-positive CCE; anti-N-methyl-D-aspartate receptor encephalitis; demyelinating disease; symptoms.
Copyright © 2023 Yang, Yang, Han, Gao and Cao.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
FLAMES overlaying anti-N-methyl-D-aspartate receptor encephalitis: a case report and literature review.BMC Neurol. 2024 Apr 25;24(1):140. doi: 10.1186/s12883-024-03617-z. BMC Neurol. 2024. PMID: 38664672 Free PMC article. Review.
-
FLAIR-hyperintense lesions in anti-MOG-associated encephalitis with seizures overlaying anti-N-methyl-D-aspartate receptor encephalitis: A case report.Medicine (Baltimore). 2023 Nov 10;102(45):e35948. doi: 10.1097/MD.0000000000035948. Medicine (Baltimore). 2023. PMID: 37960781 Free PMC article.
-
Clinical and radiological features, treatment responses and prognosis in pediatric patients with co-existing anti-N-methyl-D-aspartate receptor and myelin oligodendrocyte glycoprotein antibody-associated encephalitis: A single center study.Mult Scler Relat Disord. 2024 Jan;81:105133. doi: 10.1016/j.msard.2023.105133. Epub 2023 Nov 13. Mult Scler Relat Disord. 2024. PMID: 37984120
-
Clinical characteristics of children with anti-N-methyl-D-aspartate receptor encephalitis with and without anti-myelin oligodendrocyte glycoprotein antibody.Eur J Pediatr. 2025 Mar 14;184(4):249. doi: 10.1007/s00431-025-06078-9. Eur J Pediatr. 2025. PMID: 40082268
-
Unilateral cortical FLAIR-hyperintense Lesions in Anti-MOG-associated Encephalitis with Seizures (FLAMES): characterization of a distinct clinico-radiographic syndrome.J Neurol. 2019 Oct;266(10):2481-2487. doi: 10.1007/s00415-019-09440-8. Epub 2019 Jun 26. J Neurol. 2019. PMID: 31243540
Cited by
-
FLAIR hyperintense cortical lesions in myelin oligodendrocyte glycoprotein-associated encephalitis with seizures in children: a retrospective single-center case series.Front Immunol. 2025 Jul 16;16:1563481. doi: 10.3389/fimmu.2025.1563481. eCollection 2025. Front Immunol. 2025. PMID: 40740785 Free PMC article.
-
Efficacy of steroid therapy in the acute stage of anti-NMDAR and anti-MOG antibody overlapping encephalitis: a case report and literature review.Front Immunol. 2024 Jun 4;15:1392992. doi: 10.3389/fimmu.2024.1392992. eCollection 2024. Front Immunol. 2024. PMID: 38895128 Free PMC article. Review.
-
Successful sequential therapy with rituximab and telitacicept in refractory Anti-NMDA receptor encephalitis and MOG-associated demyelination: a case report and literature review.Front Immunol. 2025 Feb 6;16:1509143. doi: 10.3389/fimmu.2025.1509143. eCollection 2025. Front Immunol. 2025. PMID: 39981240 Free PMC article. Review.
-
FLAIR Hyperintense Cortical Lesions in a 4-Year-Old Child with Myelin Oligodendrocyte Glycoprotein (MOG)-Associated Encephalitis and Seizures: A Case Report.Children (Basel). 2024 Jun 27;11(7):778. doi: 10.3390/children11070778. Children (Basel). 2024. PMID: 39062226 Free PMC article.
-
The spectrum of overlapping anti-NMDAR encephalitis and demyelinating syndromes: a systematic review of presentation, diagnosis, management, and outcomes.Ann Med. 2025 Dec;57(1):2517813. doi: 10.1080/07853890.2025.2517813. Epub 2025 Jul 3. Ann Med. 2025. PMID: 40611612 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous