

Ultrasound-Guided Quadratus Lumborum Block at the Lateral Supra-Arcuate Ligament versus Subcostal Transversus Abdominis Plane Block for Postoperative Analgesia Following Open Hepatectomy: A Randomized Controlled Trial
- PMID: 37138955
- PMCID: PMC10150756
- DOI: 10.2147/JPR.S404810
Ultrasound-Guided Quadratus Lumborum Block at the Lateral Supra-Arcuate Ligament versus Subcostal Transversus Abdominis Plane Block for Postoperative Analgesia Following Open Hepatectomy: A Randomized Controlled Trial
Abstract
Purpose: Many studies confirmed that several approaches of quadratus lumborum block (QLB) were superior to transversus abdominis plane block (TAPB) in reducing opioid consumption during postoperative period. As a new QLB approach at the lateral supra-arcuate ligament (QLB-LSAL), the analgesic efficacy and safety in patients undergoing open hepatectomy are still unknown. This study aims to compare postoperative analgesia between the blocks in open hepatectomy.
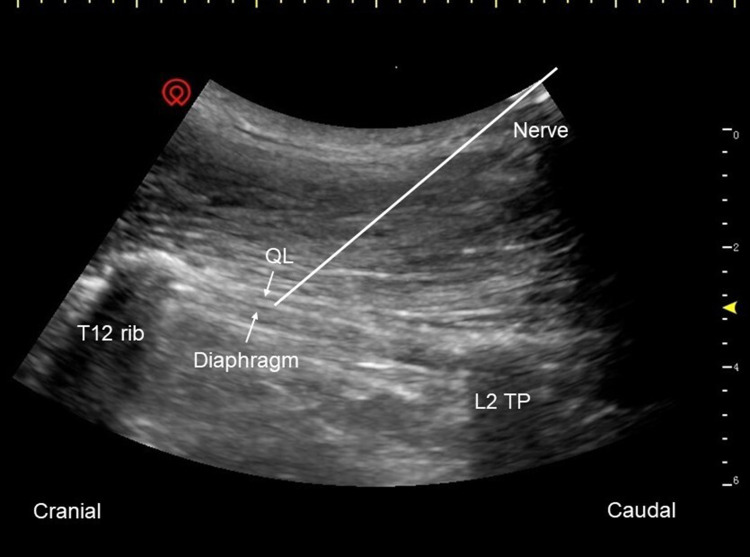
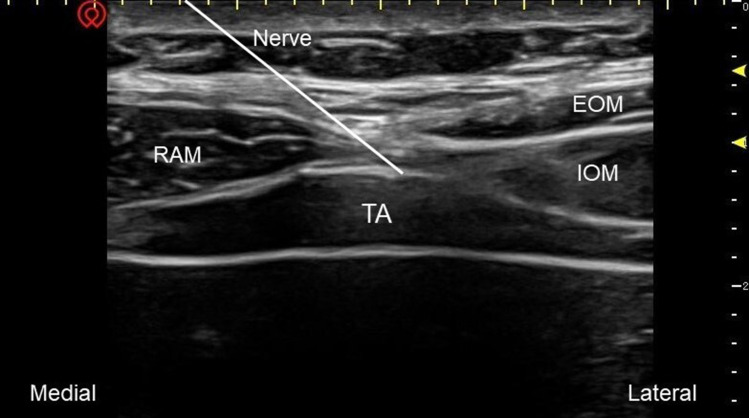
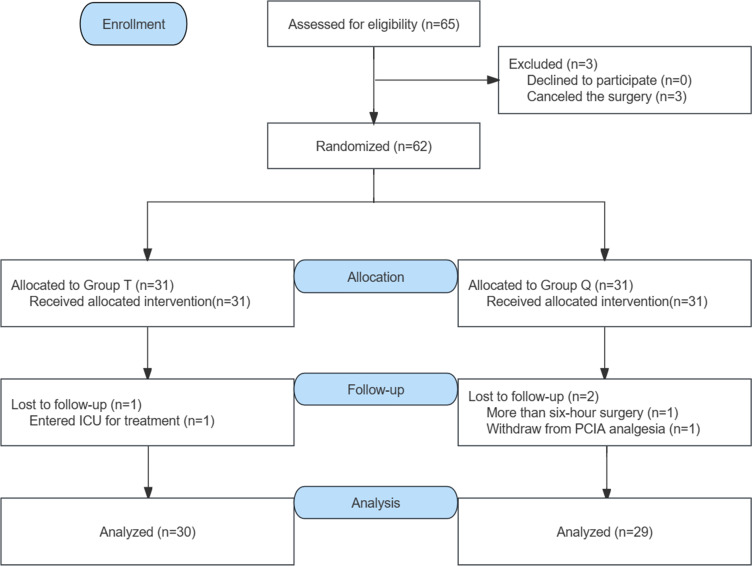
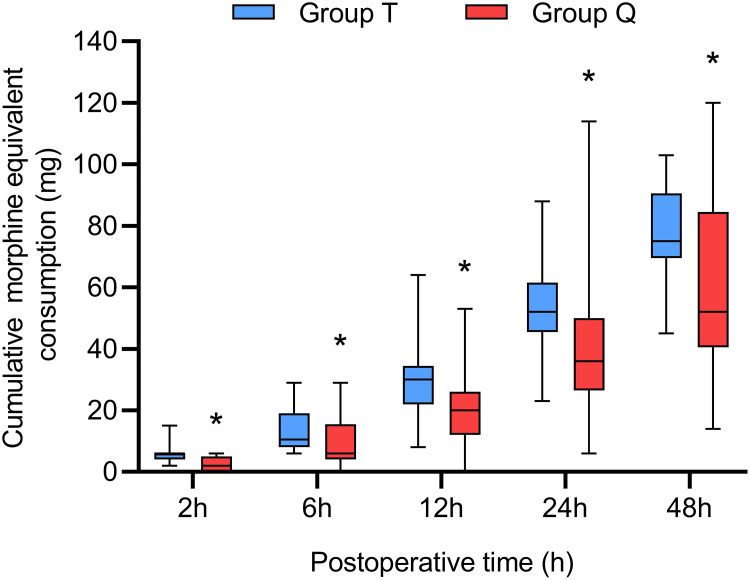
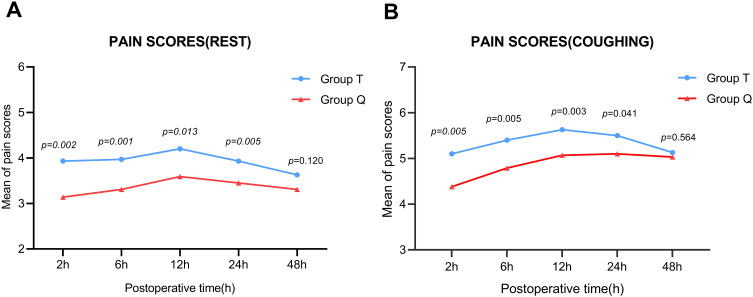
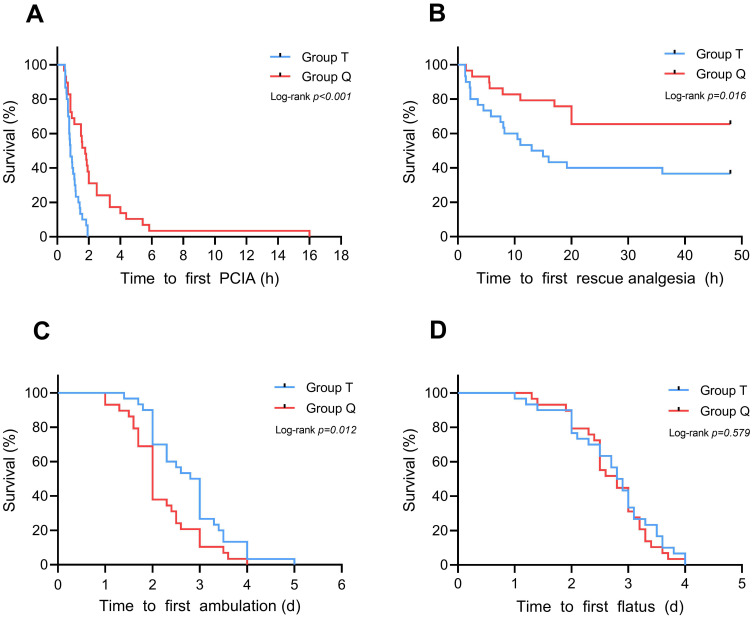
Patients and methods: Sixty-two patients undergoing open hepatectomy were enrolled and randomly allocated into the QLB-LSAL group (group Q) and the subcostal TAPB group (group T). Preoperatively, patients received ultrasound-guided bilateral QLB-LSAL or subcostal TAPB with injection of 0.5% ropivacaine (a total volume of 40 mL). The primary outcome was cumulative total morphine equivalent consumption in the first postoperative 24 h. Other outcomes included numerical rating scale (NRS) scores at rest and coughing, cumulative total morphine equivalent consumption at 2, 6, 12, 48 h, Quality of Recovery-15 (QoR-15) scores, time to first patient-controlled intravenous analgesia (PCIA) request, time to first ambulation and adverse effects.
Results: The cumulative total morphine equivalent consumption in group Q was decreased significantly at all postoperative time points (P < 0.01). The postoperative NRS scores at rest and coughing in group Q were lower than those in group T at all postoperative time points except 48 h (P < 0.05). A significant increase was also observed in the QoR-15 scores among patients in group Q. Time to first PCIA request was significantly prolonged in group Q than in group T, and time to first ambulation was shortened. Adverse effects showed no statistical significance between the two groups.
Conclusion: Compared with subcostal TAPB, preoperative bilateral QLB-LSAL provided superior analgesic properties and promoted early postoperative recovery quality in patients undergoing open hepatectomy.
Trial registration: China Clinical Trials Registration Center (http://www.chictr.org.cn) ChiCTR2200063291, 3/9/2022.
Keywords: analgesia; open hepatectomy; quadratus lumborum block; transversus abdominis plane block.
© 2023 Mao et al.
Conflict of interest statement
The authors declare no competing interests in this work.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials
