

Right ventricle to pulmonary artery coupling after transcatheter aortic valve implantation-Determinant factors and prognostic impact
- PMID: 37139141
- PMCID: PMC10150002
- DOI: 10.3389/fcvm.2023.1150039
Right ventricle to pulmonary artery coupling after transcatheter aortic valve implantation-Determinant factors and prognostic impact
Abstract
Introduction: Right ventricular (RV) dysfunction and pulmonary hypertension (PH) have been previously associated with unfavorable outcomes in patients with severe aortic stenosis (AS) undergoing transcatheter aortic valve implantation (TAVI), but little is known about the effect of right ventricle (RV) to pulmonary artery (PA) coupling. Our study aimed to evaluate the determinant factors and the prognostic value of RV-PA coupling in patients undergoing TAVI.
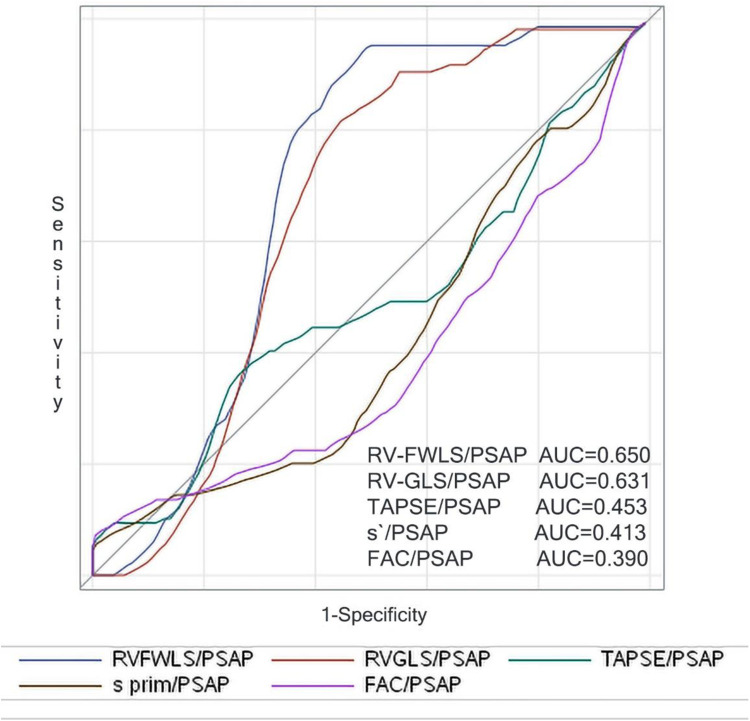
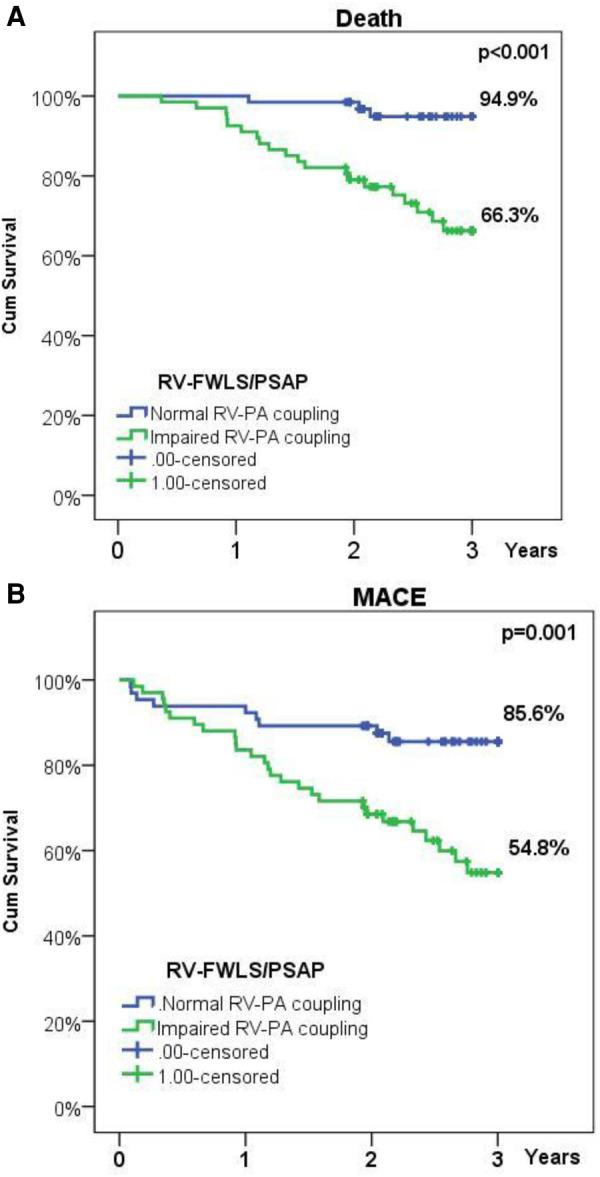
Methods: One hundred sixty consecutive patients with severe AS were prospectively enrolled, between September 2018 and May 2020. They underwent a comprehensive echocardiogram before and 30 days after TAVI, including speckle tracking echocardiography (STE) for myocardial deformation analysis of the left ventricle (LV), left atrium (LA), and RV function. Complete data on myocardial deformation was available in 132 patients (76.6 ± 7.5 years, 52.5% men) who formed the final study population. The ratio of RV free wall longitudinal strain (RV-FWLS) to PA systolic pressure (PASP) was used as an estimate of RV-PA coupling. Patients were analyzed according to baseline RV-FWLS/PASP cut-off point, determined through time-dependent ROC curve analysis, as follows: normal RV-PA coupling group (RV-FWLS/PASP ≥0.63, n = 65) and impaired RV-PA coupling group (RV-FWLS/PASP < 0.63, n = 67).
Results: A significant improvement of RV-PA coupling was observed early after TAVI (0.75 ± 0.3 vs. 0.64 ± 0.3 before TAVI, p < 0.001), mainly due to PASP decrease (p < 0.001). LA global longitudinal strain (LA-GLS) is an independent predictor of RV-PA coupling impairment before and after TAVI (OR = 0.837, p < 0.001, OR = 0.848, p < 0.001, respectively), while RV diameter is an independent predictor of persistent RV-PA coupling impairment after TAVI (OR = 1.174, p = 0.002). Impaired RV-PA coupling was associated with a worse survival rate (66.3% vs. 94.9%, p-value < 0.001) and emerged as an independent predictor of mortality (HR = 5.97, CI = 1.44-24.8, p = 0.014) and of the composite endpoint of death and rehospitalization (HR = 4.14, CI = 1.37-12.5, p = 0.012).
Conclusion: Our results confirm that relief of aortic valve obstruction has beneficial effects on the baseline RV-PA coupling, and they occur early after TAVI. Despite significant improvement in LV, LA, and RV function after TAVI, RV-PA coupling remains impaired in some patients, it is mainly related to persistent pulmonary hypertension and is associated with adverse outcomes.
Keywords: TAVI; aortic stenosis; coupling; pulmonary hypertension; right ventricle.
© 2023 Parasca, Calin, Cadil, Mateescu, Rosca, Botezatu, Enache, Beladan, Ginghina, Deleanu, Chioncel, Bubenek-Turconi, Iliescu and Popescu.
Conflict of interest statement
BAP has received research support and lecture honoraria from GE Healthcare and Hitachi-Aloka. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Nishimura RA, Otto CM, Bonow RO, Carabello BA, Erwin JP, Fleisher LA, et al. 2017 AHA/ACC focused update of the 2014 AHA/ACC guideline for the management of patients with valvular heart disease: a report of the American college of cardiology/American heart association task force on clinical practice guidelines. J Am Coll Cardiol. (2017) 70(2):252–89. 10.1016/j.jacc.2017.03.011 - DOI - PubMed
-
- Mack MJ, Leon MB, Smith CR, Miller DC, Moses JW, Tuzcu EM, et al. 5-year outcomes of transcatheter aortic valve replacement or surgical aortic valve replacement for high surgical risk patients with aortic stenosis (PARTNER 1): a randomised controlled trial. Lancet. (2015) 385(9986):2477–84. 10.1016/S0140-6736(15)60308-7 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous