

How symptoms of simple acute infections affect the SSS-8 and SSD-12 as screening instruments for somatic symptom disorder in the primary care setting
- PMID: 37139311
- PMCID: PMC10149793
- DOI: 10.3389/fpsyt.2023.1114782
How symptoms of simple acute infections affect the SSS-8 and SSD-12 as screening instruments for somatic symptom disorder in the primary care setting
Abstract
Objective: Somatic symptom disorder (SSD) is one of the most common reasons for consultations in primary care, in addition to simple acute infections. Questionnaire-based screening instruments to identify patients at high risk of SSD are thus of great clinical relevance. Although screening instruments are frequently used, it is currently unclear to what extent they are influenced by the concurrent presence of simple acute infections. Therefore, this study aimed to investigate how symptoms of simple acute infections affect the two established questionnaires as screening instruments for somatic symptom disorder in the primary care setting.
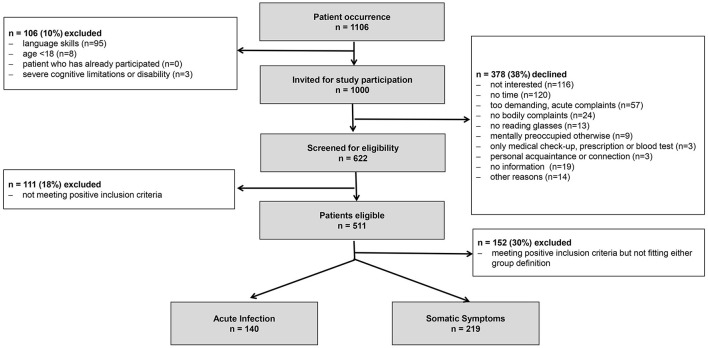
Methods: In our cross-sectional, multicenter design, a total of 1,000 patients in primary care practices were screened using the two most established SSD screening questionnaires, the 8-item Somatic Symptom Scale (SSS-8) and the 12-item Somatic Symptom Disorder-B Criteria Scale (SSD-12), followed by clinical assessment by the primary care physician.
Results: A total of 140 patients with a simple acute infection (acute infection group, AIG) and 219 patients with chronic somatic symptoms (somatic symptom group, SSG) were included. The patients in the SSG showed higher total SSS-8 and SSD-12 scores than the patients in the AIG; however, the SSS-8 was more susceptible to changes triggered by symptoms of a simple acute infection than the SSD-12.
Conclusion: These results suggest that the SSD-12 is less susceptible to symptoms of a simple acute infection. Its total score and corresponding cutoff value provide a more specific and thus less susceptible screening tool for identifying SSD in primary care.
Keywords: SSD-12; SSS-8; primary care; screening instruments; simple acute infections; somatic symptom disorder.
Copyright © 2023 Zhang, Baumeister, Spanidis, Engel, Berens, Gauss, Eich and Tesarz.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures



Similar articles
-
Detecting DSM-5 somatic symptom disorder: criterion validity of the Patient Health Questionnaire-15 (PHQ-15) and the Somatic Symptom Scale-8 (SSS-8) in combination with the Somatic Symptom Disorder - B Criteria Scale (SSD-12).Psychol Med. 2020 Jan;50(2):324-333. doi: 10.1017/S003329171900014X. Epub 2019 Feb 7. Psychol Med. 2020. PMID: 30729902
-
Detecting DSM-5 somatic symptom disorder in general hospitals in China: B-criteria instrument has better accuracy-A secondary analysis.Front Psychiatry. 2022 Oct 20;13:935597. doi: 10.3389/fpsyt.2022.935597. eCollection 2022. Front Psychiatry. 2022. PMID: 36339843 Free PMC article.
-
Identifying and measuring the severity of somatic symptom disorder using the Self-reported Somatic Symptom Scale-China (SSS-CN): a research protocol for a diagnostic study.BMJ Open. 2019 Sep 26;9(9):e024290. doi: 10.1136/bmjopen-2018-024290. BMJ Open. 2019. PMID: 31558447 Free PMC article.
-
Somatic symptom disorder in the context of Chinese yin-yang culture: A case report and literature review.Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2020 Sept 28;45(9):1142-1148. doi: 10.11817/j.issn.1672-7347.2020.200655. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2020. PMID: 33051431 Review. Chinese, English.
-
[Treatment of somatic symptom disorder in childhood: evidence-based psychotherapy interventions].Orv Hetil. 2020 Jun;161(25):1050-1058. doi: 10.1556/650.2020.31740. Orv Hetil. 2020. PMID: 32516123 Review. Hungarian.
Cited by
-
Measurement Properties of the Patient Health Questionnaire-15 and Somatic Symptom Scale-8: A Systematic Review and Meta-Analysis.JAMA Netw Open. 2024 Nov 4;7(11):e2446603. doi: 10.1001/jamanetworkopen.2024.46603. JAMA Netw Open. 2024. PMID: 39565620 Free PMC article.
-
Lessons learned from applying established cut-off values of questionnaires to detect somatic symptom disorders in primary care: a cross-sectional study.Front Psychiatry. 2024 Jan 18;14:1289186. doi: 10.3389/fpsyt.2023.1289186. eCollection 2023. Front Psychiatry. 2024. PMID: 38304401 Free PMC article.
References
-
- Grobe TG, Steinmann S, Szecseny J. Arztreport 2019 Schriftenreihe zur Gesundheitsanalyse. Berlin: Barmer; (2019). Available online at: https://www.barmer.de/resource/blob/1027172/d716a1cbc5eec45894a3f47b6214... (accessed June 03, 2022).
-
- Smith CM, Shallcross LJ, Dutey-Magni P, Conolly A, Fuller C, Hill S, et al. . Incidence, healthcare-seeking behaviours, antibiotic use and natural history of common infection syndromes in England: results from the Bug Watch community cohort study. BMC Infect Dis. (2021) 21:105. 10.1186/s12879-021-05811-7 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources