

Familial Clonal Hematopoiesis in a Long Telomere Syndrome
- PMID: 37140166
- PMCID: PMC10501156
- DOI: 10.1056/NEJMoa2300503
Familial Clonal Hematopoiesis in a Long Telomere Syndrome
Abstract
Background: Telomere shortening is a well-characterized cellular aging mechanism, and short telomere syndromes cause age-related disease. However, whether long telomere length is advantageous is poorly understood.
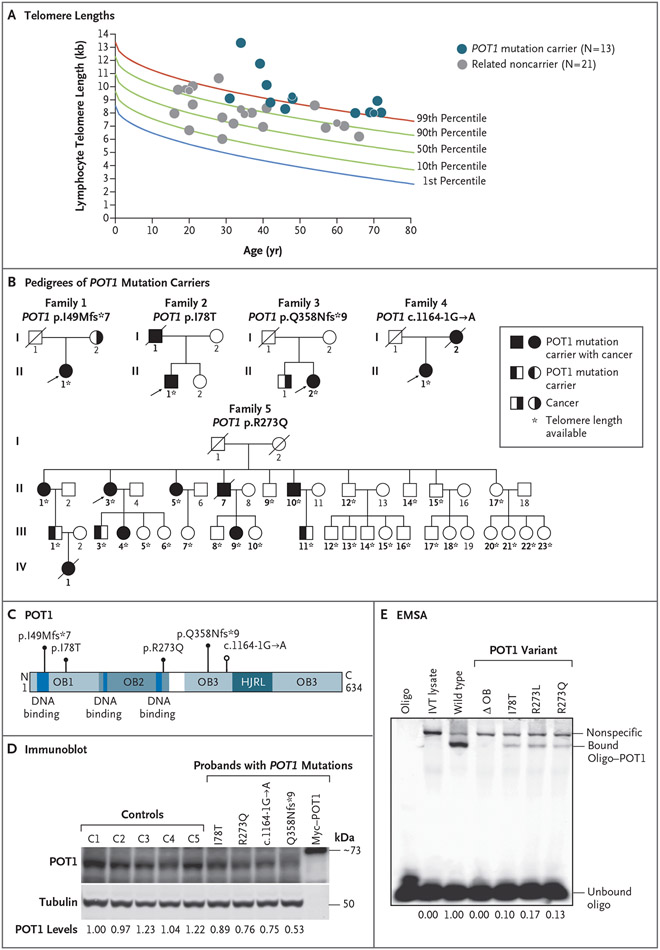
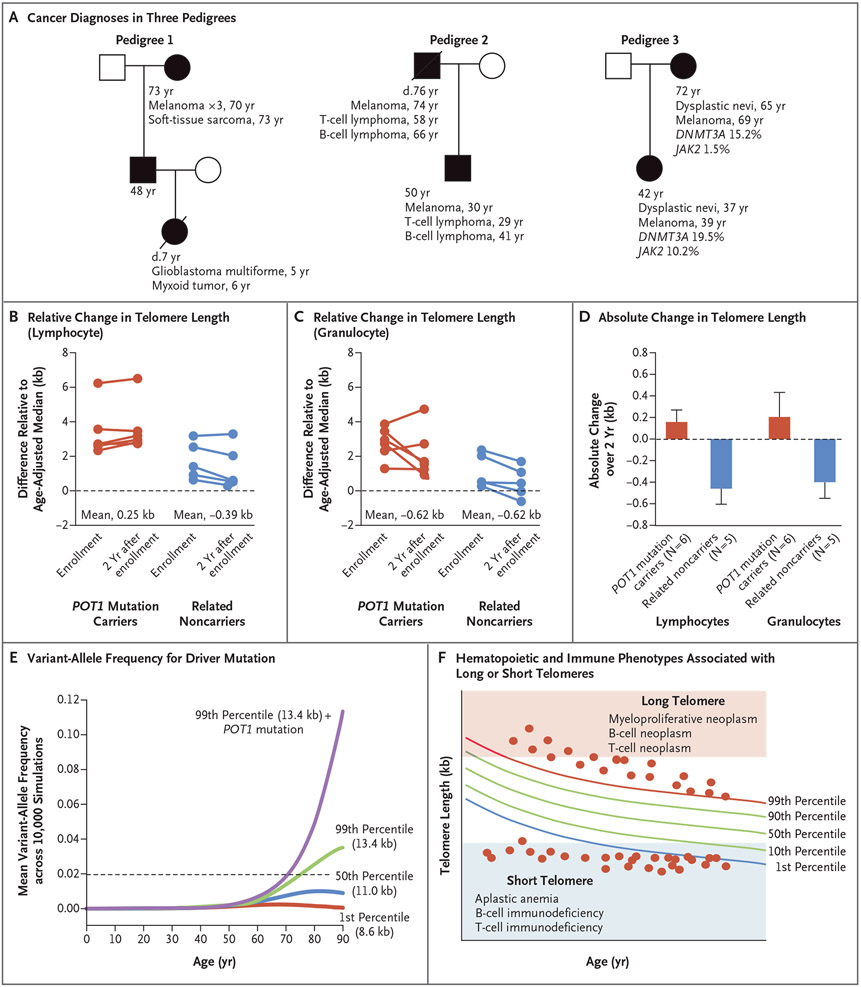
Methods: We examined the clinical and molecular features of aging and cancer in persons carrying heterozygous loss-of-function mutations in the telomere-related gene POT1 and noncarrier relatives.
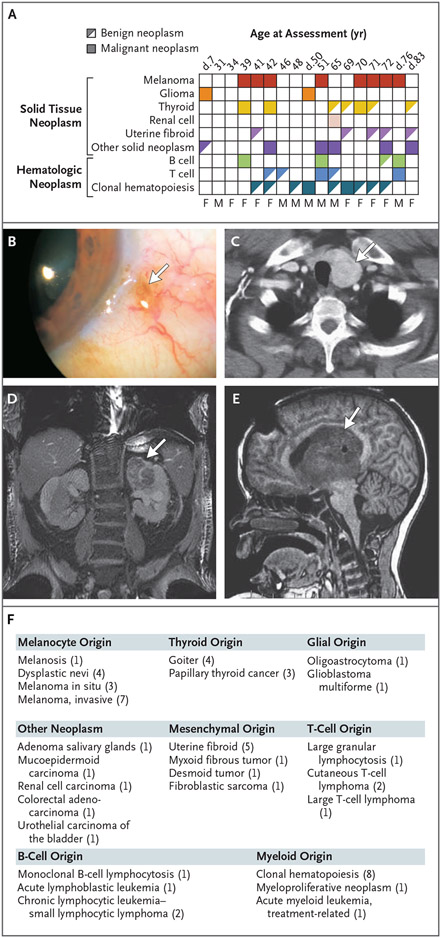
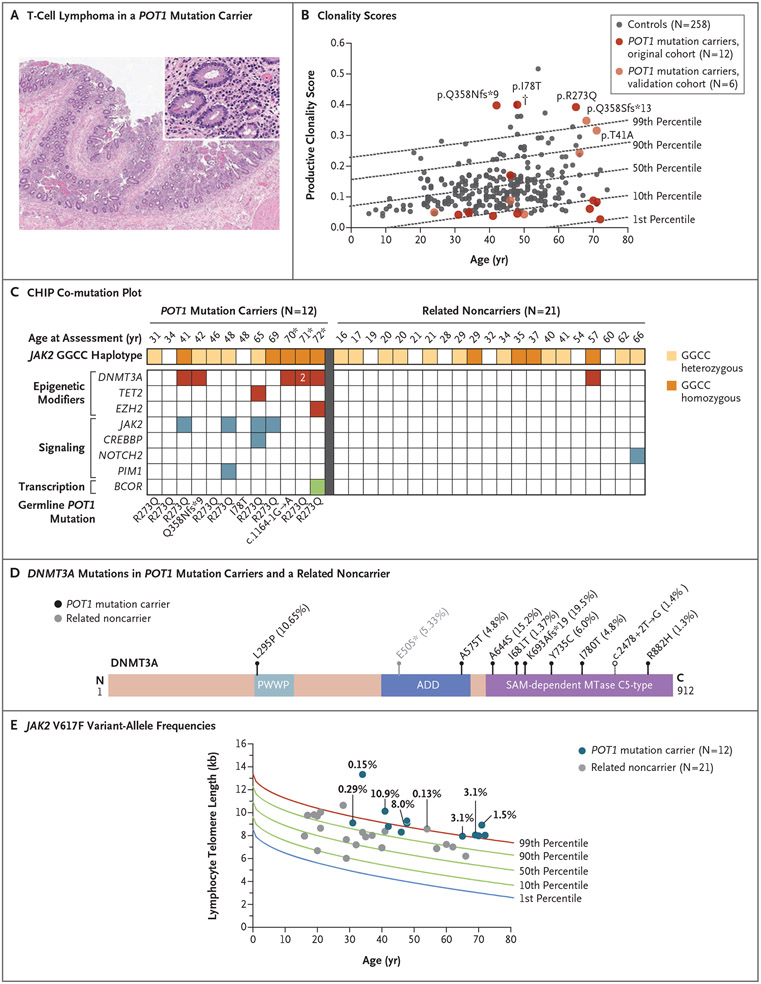
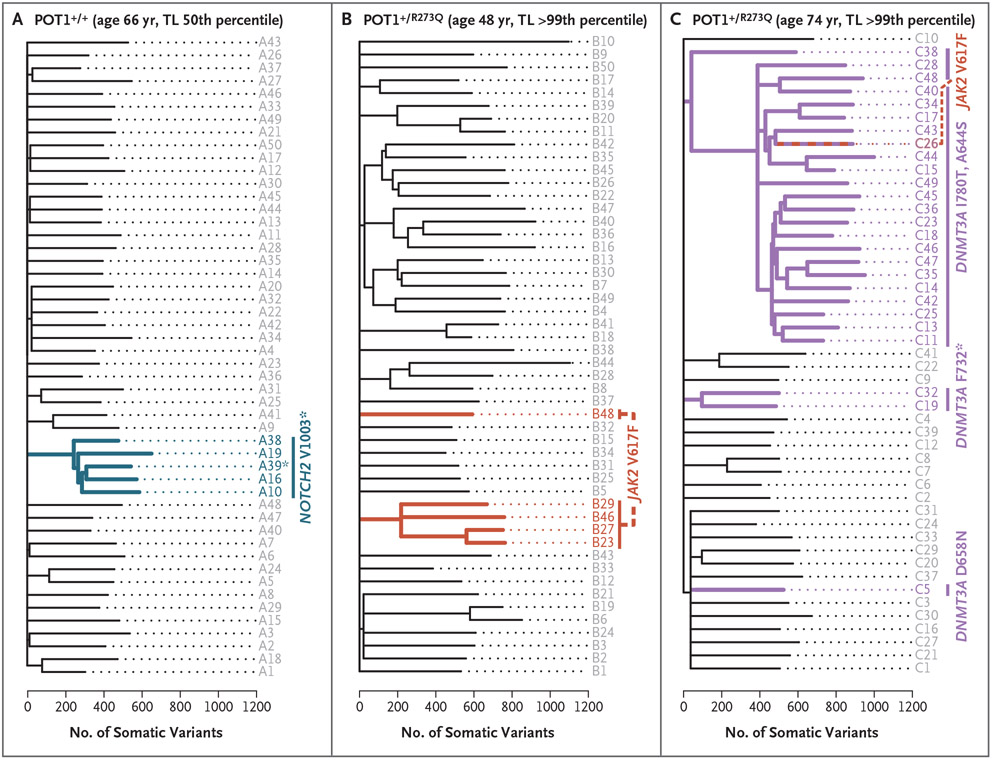
Results: A total of 17 POT1 mutation carriers and 21 noncarrier relatives were initially included in the study, and a validation cohort of 6 additional mutation carriers was subsequently recruited. A majority of the POT1 mutation carriers with telomere length evaluated (9 of 13) had long telomeres (>99th percentile). POT1 mutation carriers had a range of benign and malignant neoplasms involving epithelial, mesenchymal, and neuronal tissues in addition to B- and T-cell lymphoma and myeloid cancers. Five of 18 POT1 mutation carriers (28%) had T-cell clonality, and 8 of 12 (67%) had clonal hematopoiesis of indeterminate potential. A predisposition to clonal hematopoiesis had an autosomal dominant pattern of inheritance, as well as penetrance that increased with age; somatic DNMT3A and JAK2 hotspot mutations were common. These and other somatic driver mutations probably arose in the first decades of life, and their lineages secondarily accumulated a higher mutation burden characterized by a clocklike signature. Successive generations showed genetic anticipation (i.e., an increasingly early onset of disease). In contrast to noncarrier relatives, who had the typical telomere shortening with age, POT1 mutation carriers maintained telomere length over the course of 2 years.
Conclusions: POT1 mutations associated with long telomere length conferred a predisposition to a familial clonal hematopoiesis syndrome that was associated with a range of benign and malignant solid neoplasms. The risk of these phenotypes was mediated by extended cellular longevity and by the capacity to maintain telomeres over time. (Funded by the National Institutes of Health and others.).
Copyright © 2023 Massachusetts Medical Society.
Figures
Comment in
-
Familial Clonal Hematopoiesis in a Long Telomere Syndrome.N Engl J Med. 2023 Oct 19;389(16):1535. doi: 10.1056/NEJMc2309139. N Engl J Med. 2023. PMID: 37851887 Free PMC article. No abstract available.
-
Familial Clonal Hematopoiesis in a Long Telomere Syndrome. Reply.N Engl J Med. 2023 Oct 19;389(16):1535-1536. doi: 10.1056/NEJMc2309139. N Engl J Med. 2023. PMID: 37851888 No abstract available.
References
-
- Harley CB, Futcher AB, Greider CW. Telomeres shorten during ageing of human fibroblasts. Nature 1990;345:458–60. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous