

Lower vs Higher Fluid Volumes in Adult Patients With Sepsis: An Updated Systematic Review With Meta-Analysis and Trial Sequential Analysis
- PMID: 37142091
- PMCID: PMC10567931
- DOI: 10.1016/j.chest.2023.04.036
Lower vs Higher Fluid Volumes in Adult Patients With Sepsis: An Updated Systematic Review With Meta-Analysis and Trial Sequential Analysis
Abstract
Background: IV fluids are recommended for adults with sepsis. However, the optimal strategy for IV fluid management in sepsis is unknown, and clinical equipoise exists.
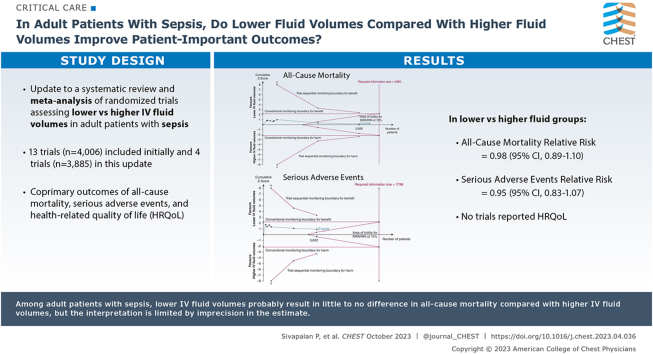
Research question: Do lower vs higher fluid volumes improve patient-important outcomes in adult patients with sepsis?
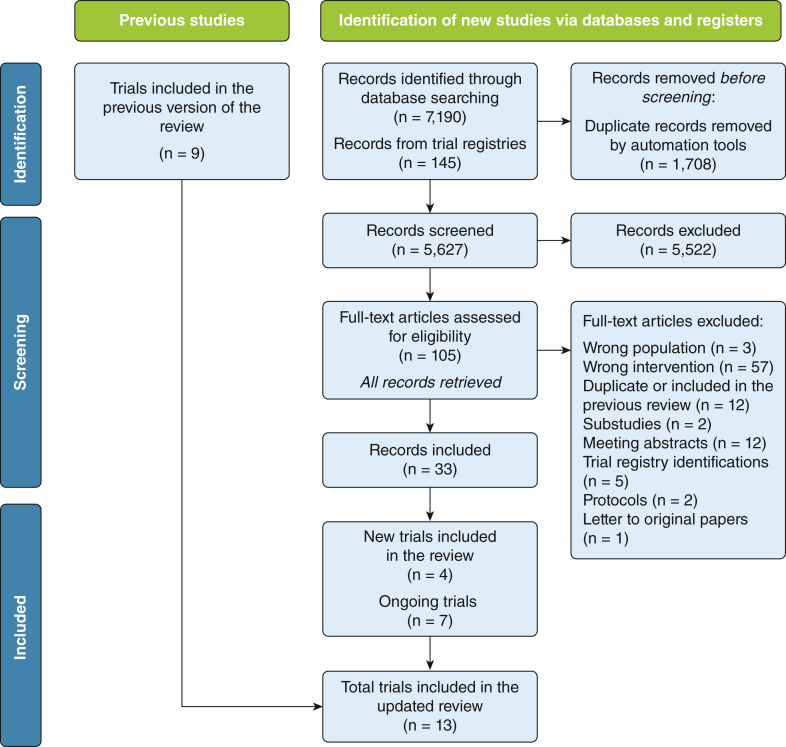
Study design and methods: We updated a systematic review with meta-analysis and trial sequential analysis of randomized clinical trials assessing lower vs higher IV fluid volumes in adult patients with sepsis. The coprimary outcomes were all-cause mortality, serious adverse events, and health-related quality of life. We followed the recommendations from the Cochrane Handbook and used the Grading of Recommendations Assessment, Development and Evaluation approach. Primary conclusions were based on trials with low risk of bias if available.
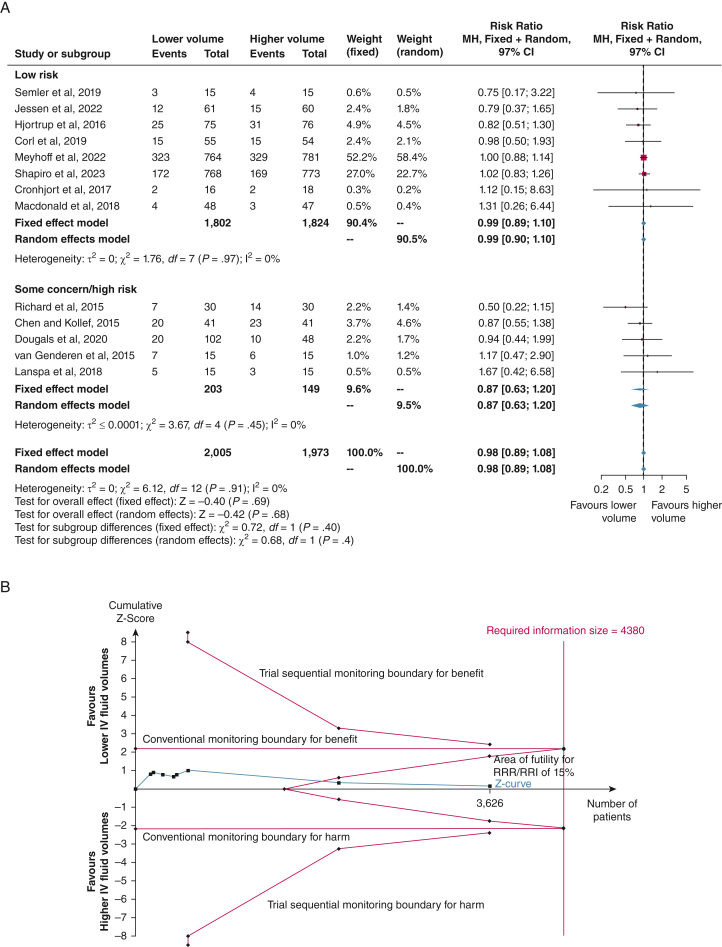
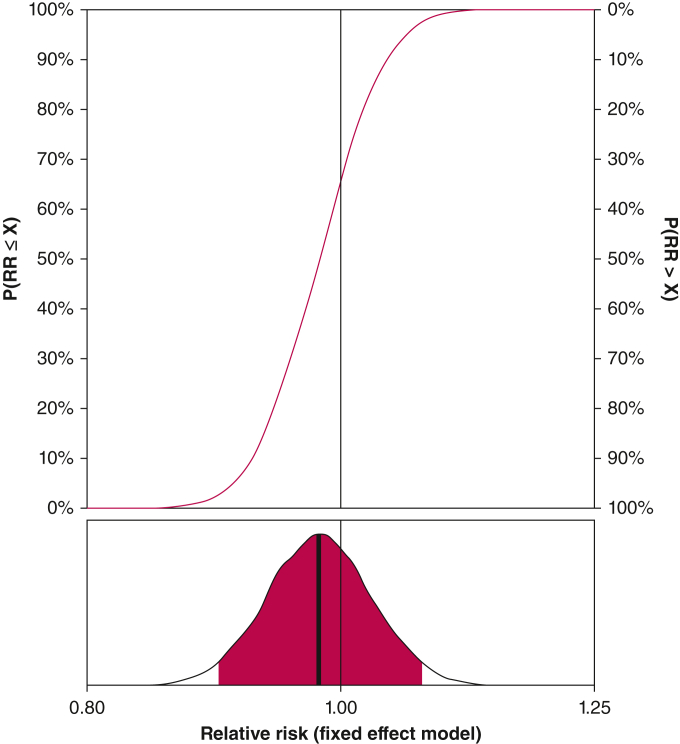
Results: We included 13 trials (N = 4,006) with four trials (n = 3,385) added to this update. The meta-analysis of all-cause mortality in eight trials with low risk of bias showed a relative risk of 0.99 (97% CI, 0.89-1.10; moderate certainty evidence). Six trials with predefined definitions of serious adverse events showed a relative risk of 0.95 (97% CI, 0.83-1.07; low certainty evidence). Health-related quality of life was not reported.
Interpretation: Among adult patients with sepsis, lower IV fluid volumes probably result in little to no difference in all-cause mortality compared with higher IV fluid volumes, but the interpretation is limited by imprecision in the estimate, which does not exclude potential benefit or harm. Similarly, the evidence suggests lower IV fluid volumes result in little to no difference in serious adverse events. No trials reported on health-related quality of life.
Trial registration: PROSPERO; No.: CRD42022312572; URL: https://www.crd.york.ac.uk/prospero/.
Keywords: fluid therapy; intensive care; sepsis; septic shock.
Copyright © 2023 The Author(s). Published by Elsevier Inc. All rights reserved.
Figures


Comment in
-
Fluid Therapy in Sepsis: Does It Matter How Much?Chest. 2023 Oct;164(4):812-813. doi: 10.1016/j.chest.2023.05.027. Chest. 2023. PMID: 37805236 No abstract available.
References
-
- Boyd J.H., Forbes J., Nakada T.A., Walley K.R., Russell J.A. Fluid resuscitation in septic shock: a positive fluid balance and elevated central venous pressure are associated with increased mortality. Crit Care Med. 2011;39(2):259–265. - PubMed
-
- Murphy C.V., Schramm G.E., Doherty J.A., et al. The importance of fluid management in acute lung injury secondary to septic shock. Chest. 2009;136(1):102–109. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
