

Talimogene laherparepvec in combination with ipilimumab versus ipilimumab alone for advanced melanoma: 5-year final analysis of a multicenter, randomized, open-label, phase II trial
- PMID: 37142291
- PMCID: PMC10163510
- DOI: 10.1136/jitc-2022-006270
Talimogene laherparepvec in combination with ipilimumab versus ipilimumab alone for advanced melanoma: 5-year final analysis of a multicenter, randomized, open-label, phase II trial
Abstract
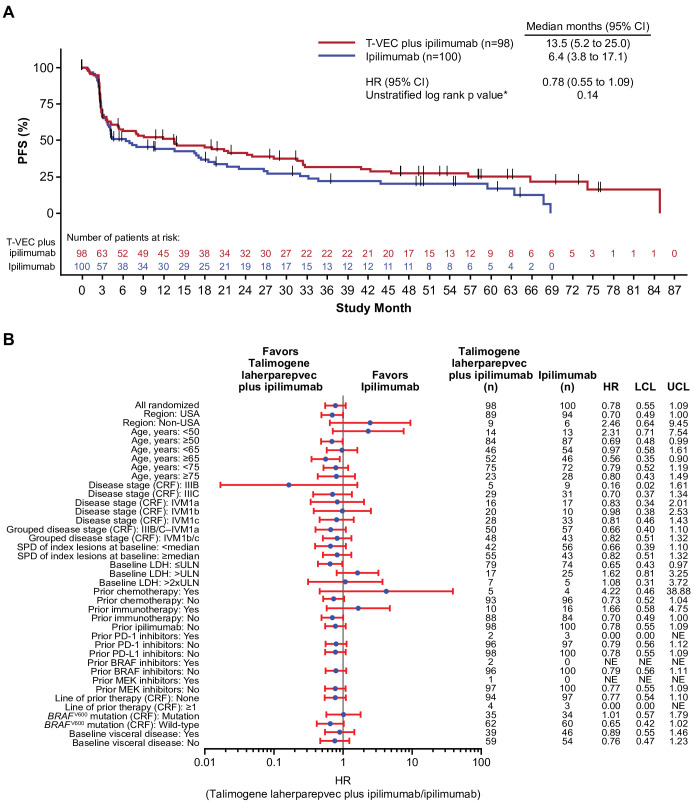
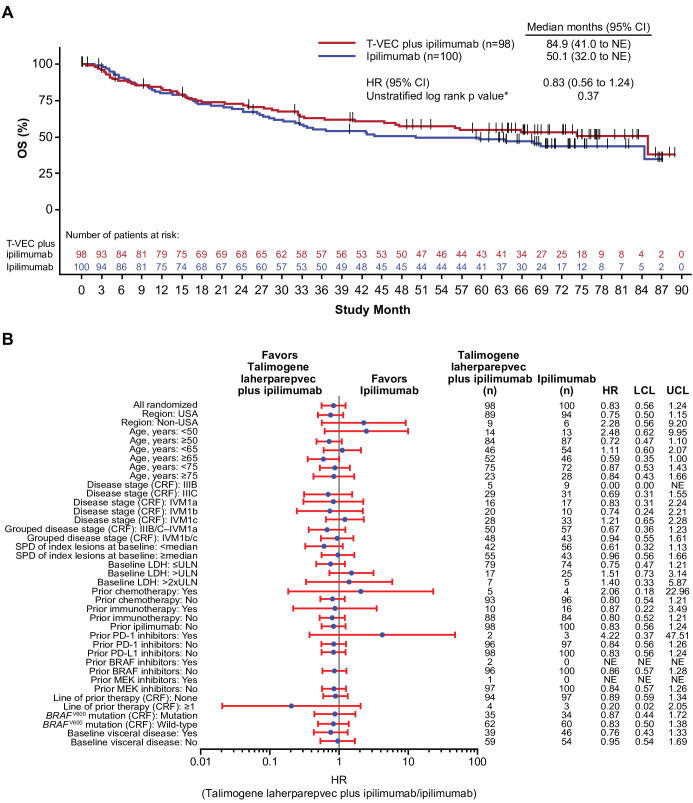
Talimogene laherparepvec (T-VEC) plus ipilimumab has demonstrated greater antitumor activity versus ipilimumab alone, without additional toxicity, in patients with advanced melanoma. Here, we report the 5-year outcomes from a randomized phase II study. These data provide the longest efficacy and safety follow-up for patients with melanoma treated with a combination of an oncolytic virus and a checkpoint inhibitor.Eligible patients with unresectable stage IIIB‒IV melanoma were randomized 1:1 to receive T-VEC plus ipilimumab or ipilimumab alone. T-VEC was administered intralesionally at 106 plaque-forming units (PFU)/mL in week 1, followed by 108 PFU/mL in week 4 and every 2 weeks thereafter. Ipilimumab (3 mg/kg every 3 weeks; ≤4 doses) was administered intravenously starting at week 1 in the ipilimumab arm and week 6 in the combination arm. The primary end point was investigator-assessed objective response rate (ORR) per immune-related response criteria; key secondary end points included durable response rate (DRR), duration of response (DOR), progression-free survival (PFS), overall survival (OS), and safety.Overall, 198 patients were randomized to receive the combination (n=98) or ipilimumab (n=100). The combination improved the ORR versus ipilimumab (35.7% vs 16.0%; OR 2.9; 95% CI 1.5 to 5.7; p=0.003). DRR was 33.7% and 13.0% (unadjusted OR 3.4; 95% CI 1.7 to 7.0; descriptive p=0.001), respectively. Among the objective responders, the median DOR was 69.2 months (95% CI 38.5 to not estimable) with the combination and was not reached with ipilimumab. Median PFS was 13.5 months with the combination and 6.4 months with ipilimumab (HR 0.78; 95% CI 0.55 to 1.09; descriptive p=0.14). Estimated 5-year OS was 54.7% (95% CI 43.9 to 64.2) in the combination arm and 48.4% (95% CI 37.9 to 58.1) in the ipilimumab arm. Forty-seven (48.0%) and 65 (65.0%) patients in the combination and ipilimumab arms, respectively, received subsequent therapies. No new safety signals were reported.At the 5-year follow-up, the improved response rates observed with T-VEC plus ipilimumab were durable. This is the first randomized controlled study of the combination of an oncolytic virus and a checkpoint inhibitor that meets its primary end point.Trial registration number: NCT01740297.
Keywords: immunotherapy; melanoma; oncolytic virotherapy; oncolytic viruses.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: JAC: research funding: Amgen, Replimune, Iovance Biotherapeutics, Bristol Myers Squibb; patents, royalties, other intellectual property: University of Louisville US Patents. IP: stock and other ownership interests: Celldex; consulting or advisory role: Amgen, Iovance Biotherapeutics, Merck, Roche, Nouscom, Seneca Therapeutics, Nektar, Oncorus. FAC: research funding: Amgen and Replimune. PS: consulting fees: Aveo, EMD Serono, Janssen, Bayer; payment or honoraria for lectures, presentations, speakers bureau, manuscript writing, or educational events: CURIO Sciences; participation on a Data Safety Monitoring Board or Advisory Board: Aveo, EMD Serono, Janssen, Bayer. MMM: consulting: Syneos, Exicure, Novartis, Immunocore, Biontech, Blueprints Medicine, Amgen, Array, Trieza. JG: funding for this trial: Amgen. OH: consultant advisor: Aduro, Akeso, Amgen, BeiGene, BioAtla, BMS, Roche Genentech, GSK, Immunocore, Idera, Incyte, Janssen, Merck, NextCure, Novartis, Pfizer, Sanofi/Regeneron, Seattle Genetics, Tempus, Zelluna; speaker bureau: BMS, Novartis, Pfizer, Sanofi/Regeneron; contracted research (for institution): Arcus, Aduro, Akeso, Amgen, BioAtla, BMS, CytomX, Exelixis, Roche Genentech, GSK, Immunocore, Idera, Incyte, Iovance, Merck, Moderna, Merck-Serono, NextCure, Novartis, Pfizer, Sanofi/Regeneron, Seattle Genetics, Torque, Zelluna. MR: honoraria: Merck and Amgen; advisory board: Merck and Amgen; research funding: Amgen and Provectus; travel funding: Merck, Amgen, Provectus, Novartis and Castle Biosciences. PF: consultant: DBV Technologies; travel to and participation on the advisory board: Castle Biosciences; stock or stock options: Gilead, Iovance. CG: personal fees: Amgen, MSD, Philogen; grants and personal fees: Novartis, NeraCare, BMS, Roche, Sanofi, outside of the submitted work. TL: funding for this trial: Amgen; grants or contracts: Abbott, Abraxis, Acceleron, Amgen, Argos, AstraZeneca, Aveo, Biovex, Bristol Myers Squibb, Eisai, Lilly, GlaxoSmithKline, Immatics, Roche, Merck, Novartis, Pfizer, Synta, Thershold, Millenium, Tracon, Cerulean, EMD Serono, Prometheus, Macrogenics, Peloton, Iovance, MedImmune, Dynavax, NiKang; consulting fees: Prometheus; payment or honoraria for lectures, presentations, speakers bureau, manuscript writing, or educational events: SITC Advances in Cancer Immunotherapy program, organizer and presented for local program in Indianapolis. Two separate programs. AH: grants and personal fees: Amgen, BMS, Eisai, Immunocore, Pfizer, MSD/Merck, Novartis Pharma, Philogen, Pierre Fabre, Regeneron, Replimune, Immunocore, Roche, Sanofi-Genzyme, Seagen, outside the submitted work. CL: Honoraria: Roche, Bristol Myers Squibb, Novartis, Amgen, MSD, Pierre Fabre, Pfizer, Incyte; consulting or advisory role: Bristol Myers Squibb, MSD, Novartis, Amgen, Roche, Merck Serono, Sanofi, Pierre Fabre; speakers bureau: Roche, Bristol Myers Squibb, Novartis, Amgen, MSD; research funding: Roche (Inst), Bristol Myers Squibb (Inst); travel, accommodations, expenses: Bristol Myers Squibb, MSD, Novartis, Sanofi, Pierre Fabre; other relationship: Avantis Medical Systems, InflaRx. HJ: employee: Parexel. WS: employee and stockholder: Amgen. JMM: stock and other ownership interests: Pfizer; honoraria: EMD Serono, Pfizer/EMD Serono; consulting or advisory role: Merck Sharp and Dohme, Celldey, Sanofi/Regeneron, Bristol Myers Squibb, Seattle Genetics, Eisai, Novartis; research funding: Amgen, AstraZeneca, Incyte, Kinnate, Macrogenics, Bristol Myers Squibb, Merck, Novartis, Regeneron; travel, accommodations, expenses: EMD Serono, Merck Sharp and Dohme, Array BioPharma, Bristol Myers Squibb.
Figures
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical