

Abiraterone acetate plus prednisolone with or without enzalutamide for patients with metastatic prostate cancer starting androgen deprivation therapy: final results from two randomised phase 3 trials of the STAMPEDE platform protocol
- PMID: 37142371
- PMCID: PMC7616864
- DOI: 10.1016/S1470-2045(23)00148-1
Abiraterone acetate plus prednisolone with or without enzalutamide for patients with metastatic prostate cancer starting androgen deprivation therapy: final results from two randomised phase 3 trials of the STAMPEDE platform protocol
Abstract
Background: Abiraterone acetate plus prednisolone (herein referred to as abiraterone) or enzalutamide added at the start of androgen deprivation therapy improves outcomes for patients with metastatic prostate cancer. Here, we aimed to evaluate long-term outcomes and test whether combining enzalutamide with abiraterone and androgen deprivation therapy improves survival.
Methods: We analysed two open-label, randomised, controlled, phase 3 trials of the STAMPEDE platform protocol, with no overlapping controls, conducted at 117 sites in the UK and Switzerland. Eligible patients (no age restriction) had metastatic, histologically-confirmed prostate adenocarcinoma; a WHO performance status of 0-2; and adequate haematological, renal, and liver function. Patients were randomly assigned (1:1) using a computerised algorithm and a minimisation technique to either standard of care (androgen deprivation therapy; docetaxel 75 mg/m2 intravenously for six cycles with prednisolone 10 mg orally once per day allowed from Dec 17, 2015) or standard of care plus abiraterone acetate 1000 mg and prednisolone 5 mg (in the abiraterone trial) orally or abiraterone acetate and prednisolone plus enzalutamide 160 mg orally once a day (in the abiraterone and enzalutamide trial). Patients were stratified by centre, age, WHO performance status, type of androgen deprivation therapy, use of aspirin or non-steroidal anti-inflammatory drugs, pelvic nodal status, planned radiotherapy, and planned docetaxel use. The primary outcome was overall survival assessed in the intention-to-treat population. Safety was assessed in all patients who started treatment. A fixed-effects meta-analysis of individual patient data was used to compare differences in survival between the two trials. STAMPEDE is registered with ClinicalTrials.gov (NCT00268476) and ISRCTN (ISRCTN78818544).
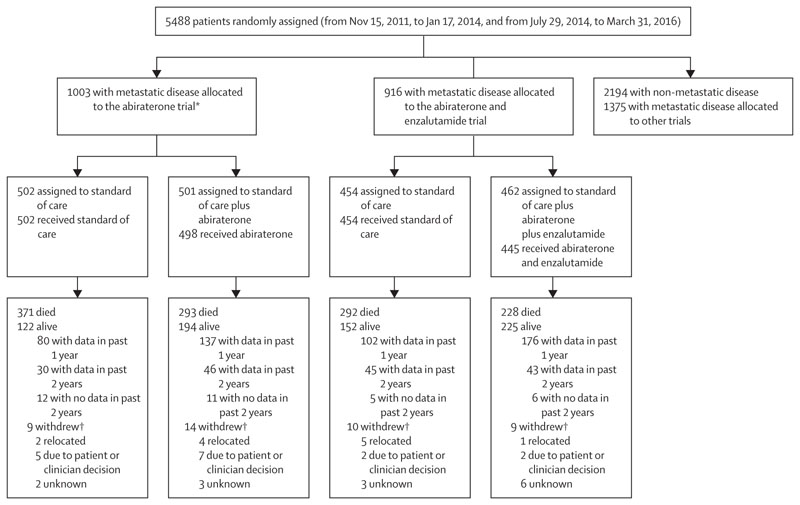
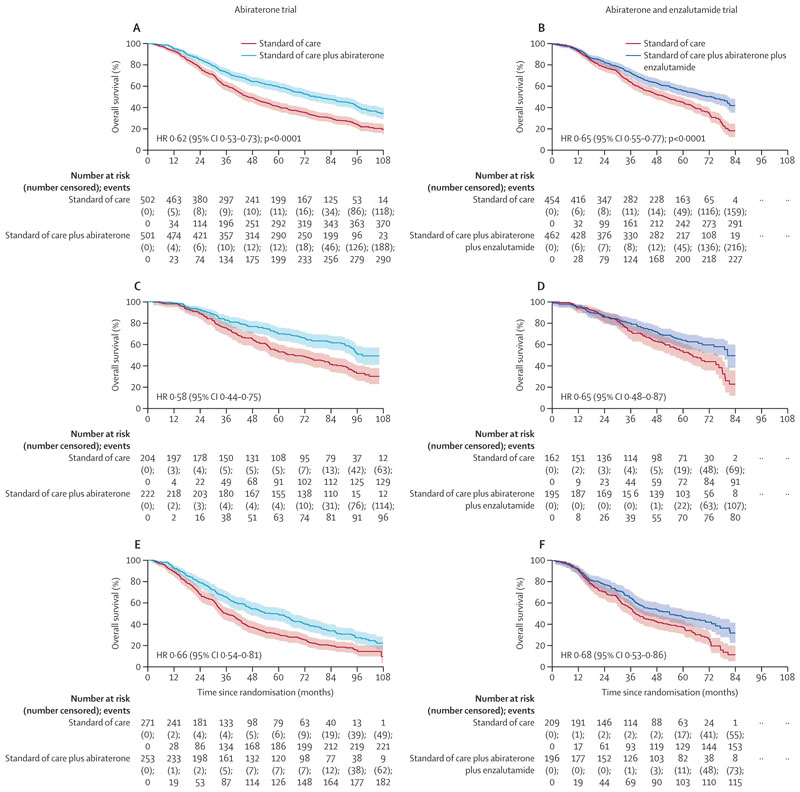
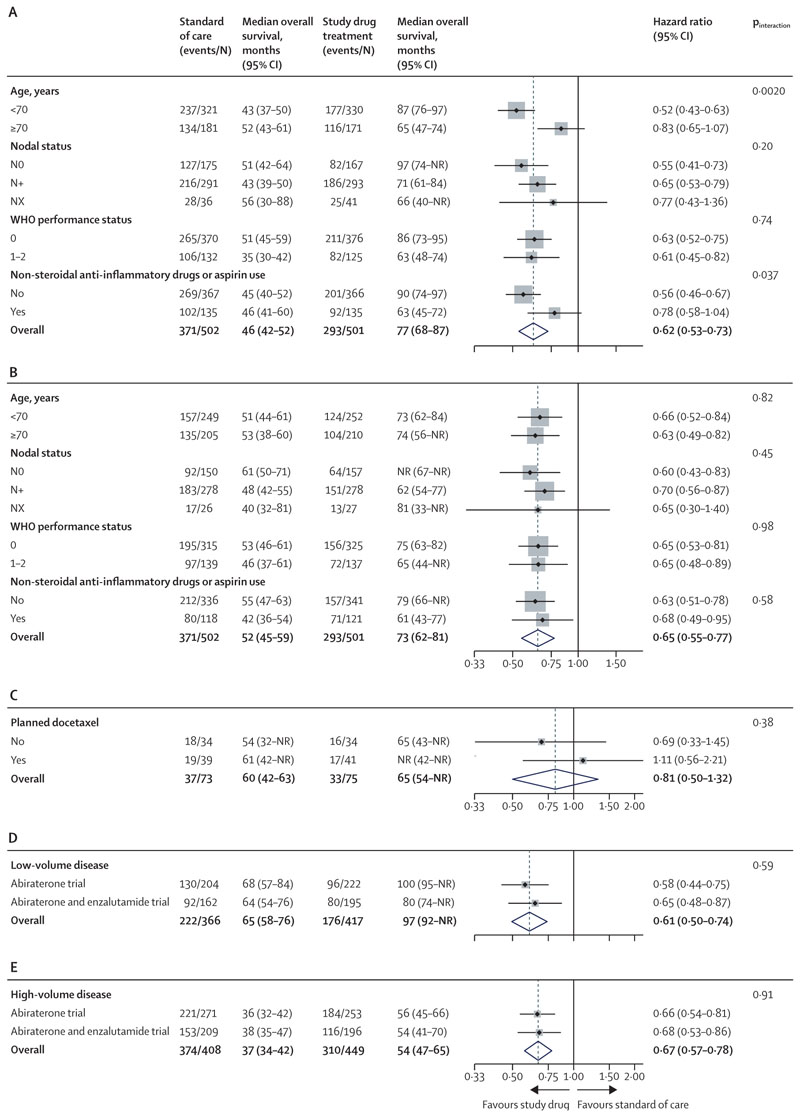
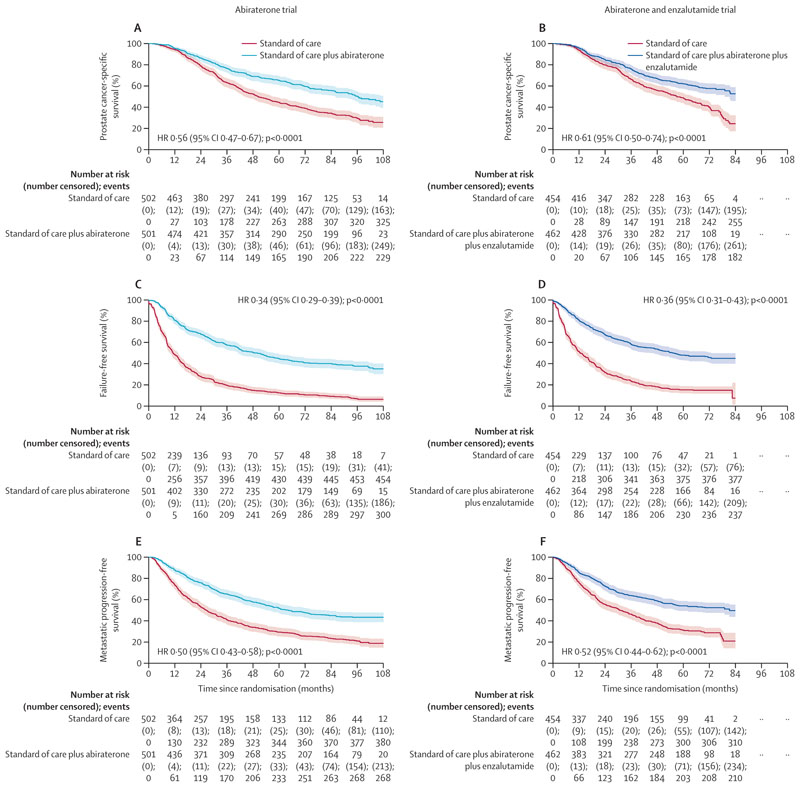
Findings: Between Nov 15, 2011, and Jan 17, 2014, 1003 patients were randomly assigned to standard of care (n=502) or standard of care plus abiraterone (n=501) in the abiraterone trial. Between July 29, 2014, and March 31, 2016, 916 patients were randomly assigned to standard of care (n=454) or standard of care plus abiraterone and enzalutamide (n=462) in the abiraterone and enzalutamide trial. Median follow-up was 96 months (IQR 86-107) in the abiraterone trial and 72 months (61-74) in the abiraterone and enzalutamide trial. In the abiraterone trial, median overall survival was 76·6 months (95% CI 67·8-86·9) in the abiraterone group versus 45·7 months (41·6-52·0) in the standard of care group (hazard ratio [HR] 0·62 [95% CI 0·53-0·73]; p<0·0001). In the abiraterone and enzalutamide trial, median overall survival was 73·1 months (61·9-81·3) in the abiraterone and enzalutamide group versus 51·8 months (45·3-59·0) in the standard of care group (HR 0·65 [0·55-0·77]; p<0·0001). We found no difference in the treatment effect between these two trials (interaction HR 1·05 [0·83-1·32]; pinteraction=0·71) or between-trial heterogeneity (I2 p=0·70). In the first 5 years of treatment, grade 3-5 toxic effects were higher when abiraterone was added to standard of care (271 [54%] of 498 vs 192 [38%] of 502 with standard of care) and the highest toxic effects were seen when abiraterone and enzalutamide were added to standard of care (302 [68%] of 445 vs 204 [45%] of 454 with standard of care). Cardiac causes were the most common cause of death due to adverse events (five [1%] with standard of care plus abiraterone and enzalutamide [two attributed to treatment] and one (<1%) with standard of care in the abiraterone trial).
Interpretation: Enzalutamide and abiraterone should not be combined for patients with prostate cancer starting long-term androgen deprivation therapy. Clinically important improvements in survival from addition of abiraterone to androgen deprivation therapy are maintained for longer than 7 years.
Funding: Cancer Research UK, UK Medical Research Council, Swiss Group for Clinical Cancer Research, Janssen, and Astellas.
Copyright © 2023 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests GA reports personal fees, grants, and travel support from Janssen and Astellas; personal fees or travel support from Pfizer, Ipsen, Novartis (Advanced Accelerator Applications), Abbott Laboratories, Ferring, ESSA Pharmaceuticals, Bayer Healthcare Pharmaceuticals, BeiGene, Takeda, AstraZeneca, and Sanofi Aventis; grant support from AstraZeneca, Innocrin Pharma, and Arno Therapeutics; receives a share of the royalty income from The Institute of Cancer Research Rewards to Discoverers Scheme for abiraterone; and holds a patent on plasma methylation signatures as biomarkers for prostate cancer (GB1915469.9). LM, AC, CB, CG, HR, CLA, CM, NP, CP, CD-M, DG, MRS, LCB, REL, and MKBP report research grants for the STAMPEDE trial from Janssen, Astellas, Novartis, Sanofi, and Clovis. NWC reports personal fees from Janssen and Astellas. AS reports grants or contracts with the National Institute for Health Research, John Black Charitable Foundation, and Prostate Cancer Foundation. RJJ reports research grants from Astellas, Clovis, Exelixis, Bayer, and Roche; and advisory board participation and speaker's honoraria from Janssen, Astellas, Bayer, Novartis, Pfizer, Merck Serono, MSD, Roche, Ipsen, and Bristol Myers Squibb. CCP reports consulting fees from Advanced Accelerator Applications, ITM Radiopharma, Myovant, and Clarity Pharmaceuticals; and speaker's honoraria from Janssen and Bayer. SG reports consulting fees from Tolremo; payment or honoraria for lectures, presentations, speaker's bureaus, manuscript writing, educational events, and honoraria from Silvio Grasso Consulting, WebMD (Medscape), European Society of Medical Oncology, Orikata, Swiss Group for Clinical Cancer Research, Beijing United Family Hospital and Clinics, Deutchland European School of Oncology, Swiss Academy of Multidisciplinary Oncology, PeerVoice, and Radiotelevisione Svizzera Italiana; travel support from Proteomedix and AstraZeneca; a patent for biomarker discovery (WO 2009138392 A1); advisory board participation for Janssen, MSD, Bayer, Roche, Astellas, Pfizer, Telixpharma, Bristol Myers Squibb, Advanced Accelerator Applications, Orion, Novartis, Modra Pharmaceuticals, AstraZeneca, Myriad Genetic, and Amgen; and a scientific committee role for Pfizer. CG reports institution funding from Astellas, Clovis Oncology, Janssen, Novartis, Pfizer, and Sanofi Genzyme; and charitable funding from Cancer Research UK and Medical Research Council. SC reports consulting fees from Telix, Novartis (Advanced Accelerator Applications), Huma, Remedy Bio, and Curesponse; payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing, or educational events from Bayer, Janssen, Astellas, Amgen, and Advanced Accelerator Applications; participation on a data safety monitoring board or advisory board for Amgen, Janssen, and Bayer; and stocks in Huma and Remedy Bio. JMO reports a grant from Prostate Cancer UK. AB reports speaker's fees from Janssen, Astellas, Bristol Myers Squibb, Roche, MSD, and Bayer; support for attending meetings and travel from Janssen and Bayer; and participation on a data safety monitoring board or advisory board for Janssen, Bristol Myers Squibb, and AstraZeneca. NS reports support for travel expenses from Janssen-Cilag. JT reports support from Janssen and Astellas for conference attendance; and participation in advisory boards for Janssen and Astellas. PD reports payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing, or educational events from Pfizer, Bristol Myers Squibb, Ipsen, EUSA Pharma, and EISAI; support for attending meetings or travel from Janssen and Ipsen; and participation on a data safety monitoring board or advisory board for Pfizer and EUSA Pharma. OP reports support for educational meetings and conference attendance from Janssen and Astellas. AR reports sponsorships for attending a conference from Janssen. AHM reports sponsorship to attend an educational meeting from Astellas. RC reports consulting fees from Astellas, Bayer, Novartis, Janssen, Sanofi, Pfizer, MSD, Bristol Myers Squibb, Roche, Debiopharm, AstraZeneca, Ipsen, and Merck; payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing, or educational events from Ipsen, Astellas, Janssen, Roche, and Merck; and participation as a board member for the Swiss Group for Clinical Cancer Research. DPD reports consulting fees and participation on an advisory board for Janssen; and a patent for a localisation and stabilisation device (EP1933709B1). MRS reports speaker fees from Eisai and being a non-paid member of independent data monitoring committees for academic sponsors. NDJ reports research grants for the STAMPEDE trial from Janssen, Astellas, Novartis, Sanofi, Clovis, and Cancer Research UK; and consulting and lecture fees from Astellas and Janssen. All other authors declare no competing interests.
Figures
Comment in
-
Metastatic prostate cancer management: 20 years of progress.Lancet Oncol. 2023 May;24(5):416-417. doi: 10.1016/S1470-2045(23)00167-5. Lancet Oncol. 2023. PMID: 37142365 No abstract available.
References
-
- James ND, Spears MR, Clarke NW, et al. Survival with newly diagnosed metastatic prostate cancer in the “docetaxel era”: data from 917 patients in the control arm of the STAMPEDE trial (MRC PR08, CRUK/06/019. Eur Urol. 2015;67:1028–38. - PubMed
-
- James ND, Sydes MR, Clarke NW, et al. Addition of docetaxel, zoledronic acid, or both to first-line long-term hormone therapy in prostate cancer (STAMPEDE): survival results from an adaptive, multiarm, multistage, platform randomised controlled trial. Lancet. 2016;387:1163–77. doi: 10.1016/S0140-6736(15)01037-5. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
