

Acupuncture for post-stroke depression: a systematic review and network meta-analysis
- PMID: 37143014
- PMCID: PMC10161596
- DOI: 10.1186/s12888-023-04749-1
Acupuncture for post-stroke depression: a systematic review and network meta-analysis
Abstract
Background: Patients with post-stroke depression (PSD) usually experience anxiety, hopelessness, and insomnia, which have a negative impact on their daily activities and post-stroke rehabilitation. Acupuncture (AC), as a minimally invasive technique, has become a popular choice for improving depression symptoms. However, it is still unclear which therapy is associated with the best outcomes for PSD. In this review, we aimed to explore the impact of AC in alleviating symptoms of PSD and to evaluate the difference in effectiveness between AC combined with pharmacotherapies and various non-pharmacotherapies.
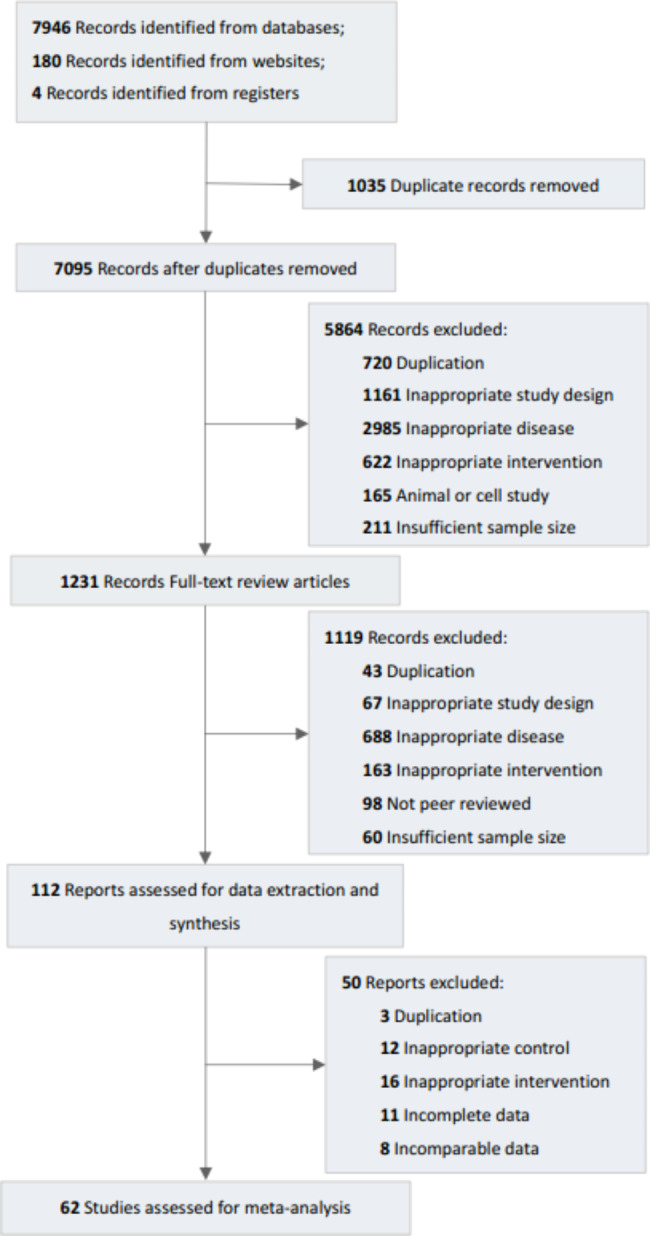
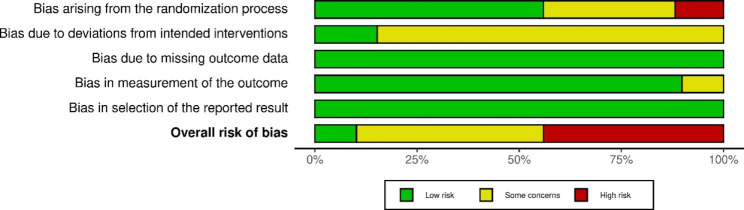
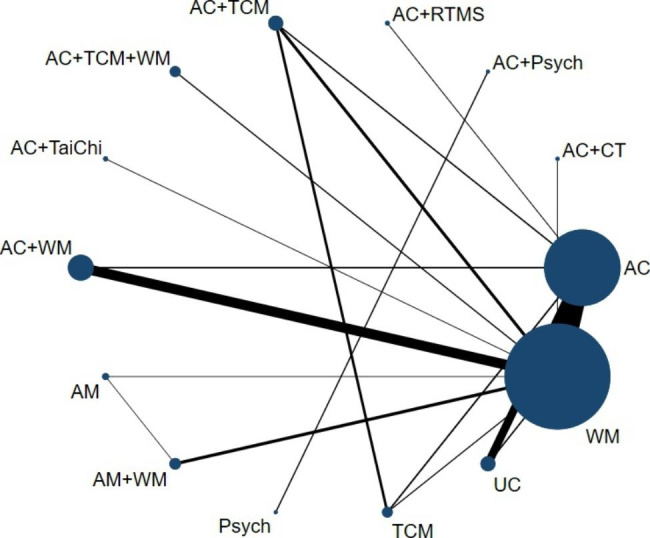
Methods: Six databases and three clinical trials registration platforms were searched from inception to March 2023. Randomized clinical trial comparing needle-based AC with pharmacotherapy, and other non-pharmacotherapy or invalid group were included. Two independent reviewers identified eligible studies, and collected data using a pre-made form. A Bayesian network meta-analysis was conducted to assess and compare different techniques using RStudio 3.6.0 with the package 'GEMTC' V.0.8.1. The primary outcome was the efficacy for PSD assessed by scales measuring depressive symptoms. The secondary outcomes were effectiveness for neurological function and the quality of life. The ranking probabilities for all treatment interventions was performed using the Surface Under the Cumulative Ranking curve (SUCRA). The risk of bias was assessed by using the Revised Cochrane Risk of Bias tool 2.
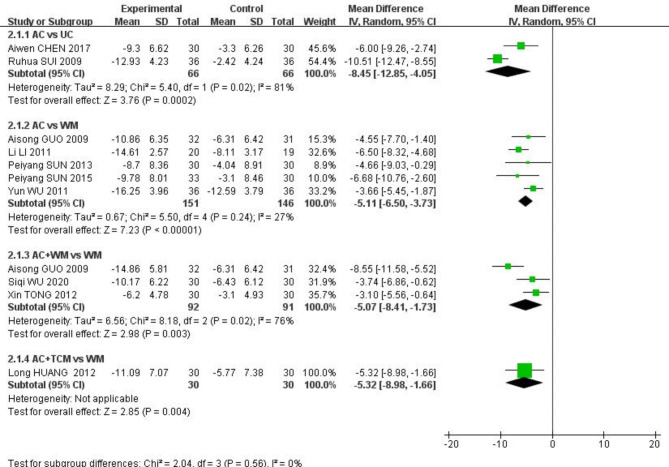
Results: Sixty-two studies, involving 5308 participants published from 2003 to 2022, were included. The results showed that compared with western medicine (WM) (defined as pharmacotherapy for PSD), AC alone or with repetitive transcranial magnetic stimulation (RTMS), Traditional Chinese medicine (TCM) alone or with WM, were superior for alleviating depression symptoms. Compared to Usual Care, AC alone or plus other therapies could significantly decrease scores on the Hamilton Depression Rating scale. According to result of SUCRA, AC plus RTMS had the highest probability of improving depressive symptoms with a probability of 49.43%.
Conclusions: The results of this study indicate that AC alone or combined with other therapies appears to be effective in improving depression symptoms of stroke survivors. Moreover, in comparison to WM, AC alone or plus RTMS, TCM, TCM with WM, or WM, were more effective in improving depression symptoms of PSD. Also, AC with RTMS seems to be the most effective with the highest probability.
Registration: This study was registered in the International Prospective Register of Systematic Reviews (PROSPERO) database in November 2020 and updated in July 2021. The registration number is CRD42020218752.
Keywords: Acupuncture; Network meta-analysis; Post-stroke depression.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Feigin VL, Brainin M, Norrving B, Martins S, Sacco RL, Hacke W, Fisher M, Pandian J, Lindsay P. World Stroke Organization (WSO): global stroke fact sheet 2022. Int J Stroke. 2022 Jan;17(1):18–29. 10.1177/17474930211065917. - PubMed
-
- Weaver NA, Kuijf HJ, Aben HP, Abrigo J, Bae HJ, Barbay M, et al. Strategic infarct locations for post-stroke cognitive impairment: a pooled analysis of individual patient data from 12 acute ischaemic stroke cohorts. Lancet Neurol. 2021;20(6):448–59. doi: 10.1016/S1474-4422(21)00060-0. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
