

Heterogeneity in the definition of delirium in ICUs and association with the intervention effect in randomized controlled trials: a meta-epidemiological study
- PMID: 37143091
- PMCID: PMC10161412
- DOI: 10.1186/s13054-023-04411-y
Heterogeneity in the definition of delirium in ICUs and association with the intervention effect in randomized controlled trials: a meta-epidemiological study
Abstract
Purpose: To evaluate the heterogeneity in the definition of delirium in randomized controlled trials (RCTs) included in meta-analyses of delirium in intensive care units (ICUs) and to explore whether intervention effect depends on the definition used.
Methods: We searched PubMed for meta-analyses including RCTs evaluating prevention or treatment strategies of delirium in ICU. The definition of delirium was collected from RCTs and classified as validated (DSM criteria, CAM-ICU, ICDSC, NEECHAM, DRS-R98) or non-validated (non-validated scales, set of symptoms, physician appreciation or not reported). We conducted a meta-epidemiological analysis to compare intervention effects between trials using or not a validated definition by a two-step method as primary analysis and a multilevel model as secondary analysis. A ratio of odds ratios (ROR) < 1 indicated larger intervention effects in trials using a non-validated definition.
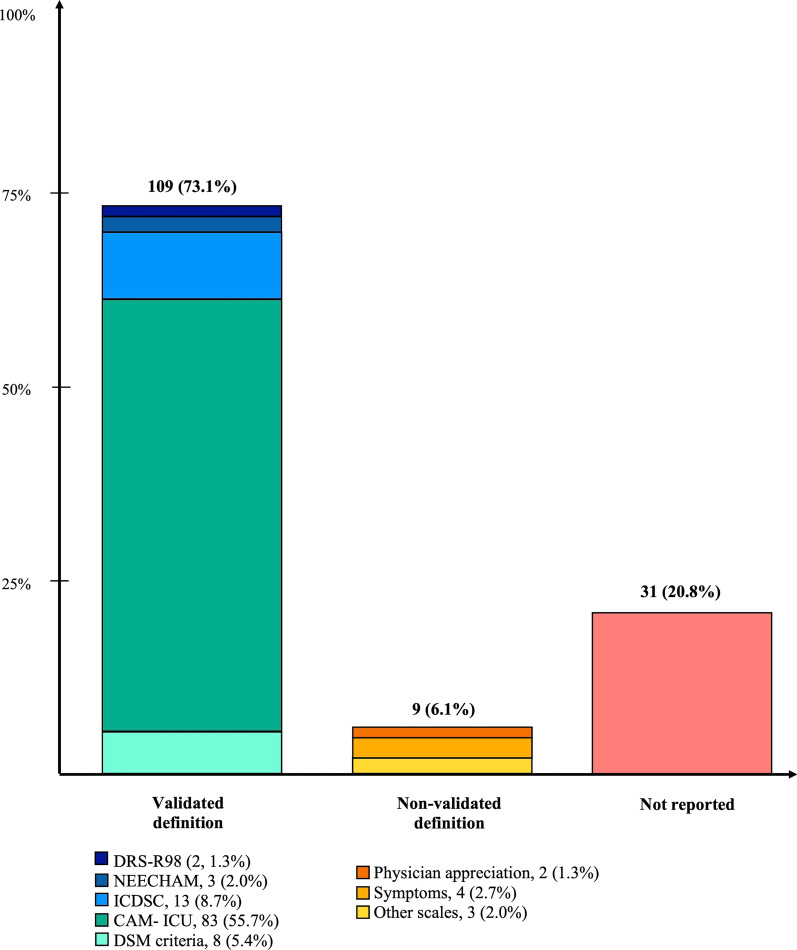
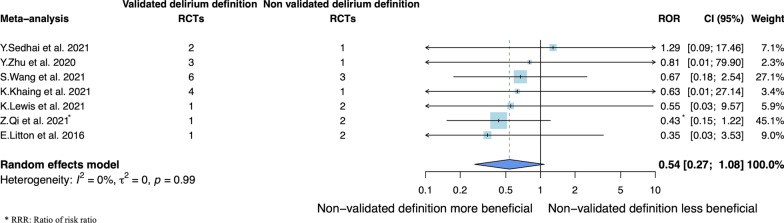
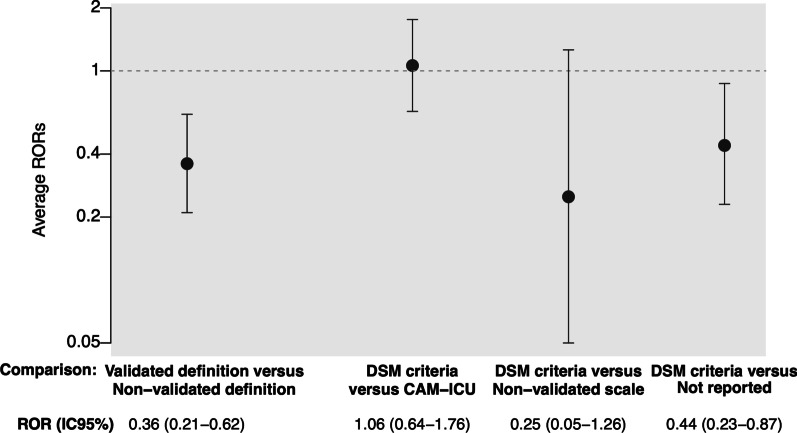
Results: Of 149 RCTs (41 meta-analyses), 109 (73.1%) used a validated definition and 40 (26.8%) did not (including 31 [20.8%] not reporting the definition). The primary analysis of 7 meta-analyses (30 RCTs) found no significant difference in intervention effects between trials using a validated definition and the others (ROR = 0.54, 95% CI 0.27-1.08), whereas the secondary multilevel analysis including 12 meta-analyses (67 RCTs) found significantly larger effects for trials using a non-validated versus a validated definition (ROR = 0.36, 95% CI 0.21-0.62).
Conclusion: The definition of delirium was heterogeneous across RCTs, with one-fifth not reporting how they evaluated delirium. We did not find a significant association with intervention effect in the primary analysis. The secondary analysis including more studies revealed significantly larger intervention effects in trials using a non-validated versus a validated definition.
Keywords: Definition; Delirium; Heterogeneity; Intensive care; Meta-analysis; Meta-epidemiology.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
