

Anterior Descending Coronary Artery Pseudoaneurysm in an 85-Year-Old Male Hemodialysis Patient: A Surgical Case Report
- PMID: 37143323
- PMCID: PMC10168633
- DOI: 10.12659/AJCR.939200
Anterior Descending Coronary Artery Pseudoaneurysm in an 85-Year-Old Male Hemodialysis Patient: A Surgical Case Report
Abstract
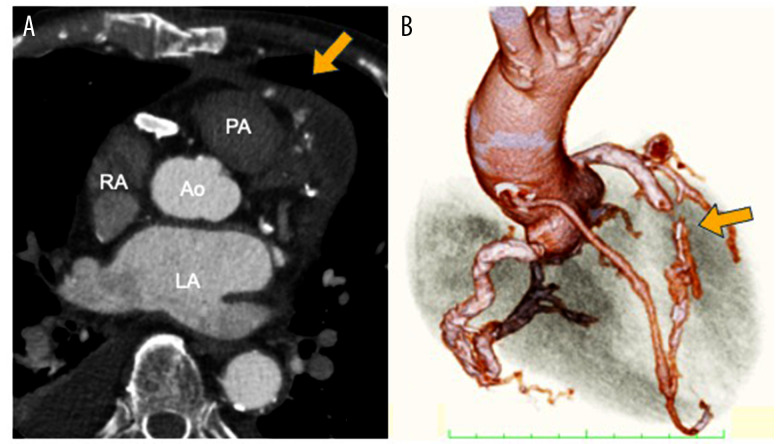
BACKGROUND Coronary artery pseudoaneurysm is an extremely rare condition. In this report, we describe an 85-year-old hemodialysis male patient who developed a coronary artery pseudoaneurysm due to physical damage associated with coronary artery calcification. CASE REPORT An 85-year-old man on hemodialysis had undergone emergency percutaneous coronary intervention of the left anterior descending artery for acute coronary syndrome 9 years ago. He presented to the emergency room with a fever and chest pain and was admitted to the cardiology department with a urinary tract infection and acute coronary syndrome. On day 21 after admission, when the urinary tract infection had resolved, coronary angiography was performed, which revealed a pseudoaneurysm proximal to the left anterior descending artery stent. The patient was scheduled to undergo surgery due to the pseudoaneurysm's risk of rupture. Surgical manipulation was performed under cardiac arrest using the median sternotomy approach. A highly calcified coronary intima was found inside the pseudoaneurysm, which was completely ruptured on the proximal side of the pseudoaneurysm. The pseudoaneurysm was closed after endarterectomy. A coronary artery bypass graft was also performed in the great saphenous vein graft of the left anterior descending artery. Histopathological examination showed no obvious signs of infection, and a diagnosis of pseudoaneurysm was established. Postoperative contrast-enhanced computed tomography showed patency of the coronary artery bypass graft and no pseudoaneurysm recurrence. CONCLUSIONS Coronary artery pseudoaneurysms are extremely rare, but this case demonstrates that atherosclerotic changes can lead to the formation of a pseudoaneurysm in an elderly hemodialysis patient.
Conflict of interest statement
Figures



Similar articles
-
Surgical repair of a pseudoaneurysm derived from a nine-year-old saphenous vein graft after coronary artery bypass.Jpn J Thorac Cardiovasc Surg. 2002 Mar;50(3):129-32. doi: 10.1007/BF02913476. Jpn J Thorac Cardiovasc Surg. 2002. PMID: 11968722
-
Percutaneous closure of a coronary artery-to-vein graft anastomotic pseudoaneurysm presenting as acute coronary syndrome after recent coronary artery bypass grafting.Tex Heart Inst J. 2015 Jun 1;42(3):265-9. doi: 10.14503/THIJ-14-4102. eCollection 2015 Jun. Tex Heart Inst J. 2015. PMID: 26175645 Free PMC article.
-
Ruptured mycotic reverse saphenous vein graft aneurysm: A late complication of mediastinitis.J Pak Med Assoc. 2020 Oct;70(10):1848-1850. doi: 10.5455/JPMA.301599. J Pak Med Assoc. 2020. PMID: 33159767
-
Giant coronary artery pseudoaneurysm causing pulmonary artery obstruction: a rare complication of coronary bypass surgery--a case report.Angiology. 1997 Dec;48(12):1073-8. doi: 10.1177/000331979704801209. Angiology. 1997. PMID: 9404835 Review.
-
Pseudoaneurysm of aortocoronary vein graft secondary to late venous rupture: case report and literature review.Br Heart J. 1993 Aug;70(2):189-92. doi: 10.1136/hrt.70.2.189. Br Heart J. 1993. PMID: 8038033 Free PMC article. Review.
Cited by
-
"No-Touch" Saphenous Vein Grafting and Coronary Aneurysm Ligation in an Adult Patient with Suspected Prior Kawasaki Disease.Am J Case Rep. 2024 Oct 6;25:e945431. doi: 10.12659/AJCR.945431. Am J Case Rep. 2024. PMID: 39369268 Free PMC article.
References
-
- Kar S, Webel RR. Diagnosis and treatment of spontaneous coronary artery pseudoaneurysm: Rare anomaly with potentially significant clinical implications. Catheter Cardiovasc Interv. 2017;90:589–97. - PubMed
-
- Cotran RS, Kumar V, Collins T, editors. Robbins pathologic basis of disease. 6th ed. Philadelphia: W.B. Saunders; 1999.
-
- Flum DR, McGinn JT, Tyras DH, Wallack MK. Coronary pseudoaneurysm after angioplasty. Am Surg. 1995;61:1035–38. - PubMed
-
- Mohara J, Konishi H, Kato M, et al. Saphenous vein graft pseudoaneurysm rupture after coronary artery bypass grafting. Ann Thorac Surg. 1998;65:831–32. - PubMed
-
- Miwa K, Matsubara T, Yasuda T, et al. Spontaneous healing of posttraumatic focal coronary aneurysm: A case report. Heart Lung. 2012;41:613–16. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
