

Surgical treatment for recurrent cholangiocarcinoma: a single-center series
- PMID: 37143948
- PMCID: PMC10152064
- DOI: 10.3389/fonc.2023.1169133
Surgical treatment for recurrent cholangiocarcinoma: a single-center series
Abstract
Purpose: The present study aims to assess the results obtained after surgical treatment of cholangiocarcinoma (CC) recurrences.
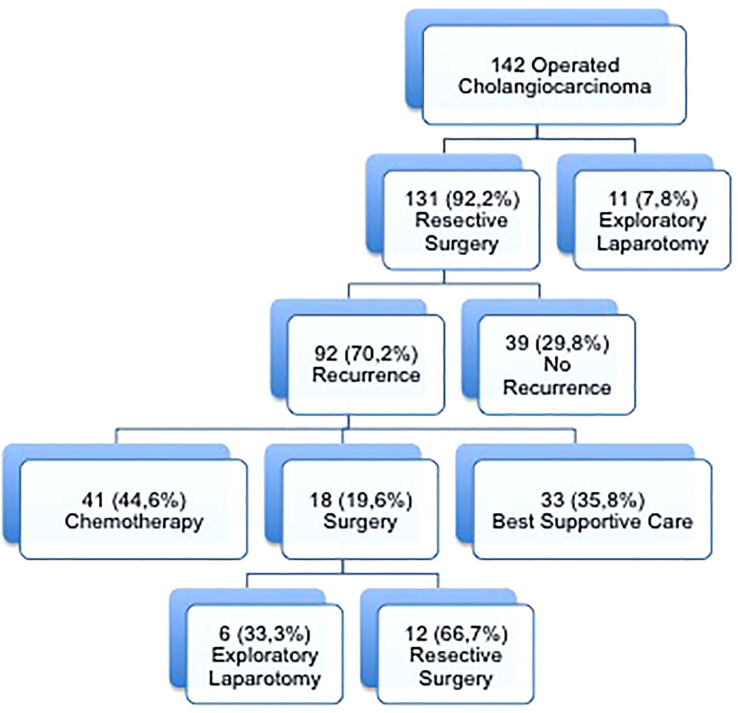
Methods: We carried out a single-center retrospective study, including all patients with recurrence of CC. The primary outcome was patient survival after surgical treatment compared with chemotherapy or best supportive care. A multivariate analysis of variables affecting mortality after CC recurrence was performed.
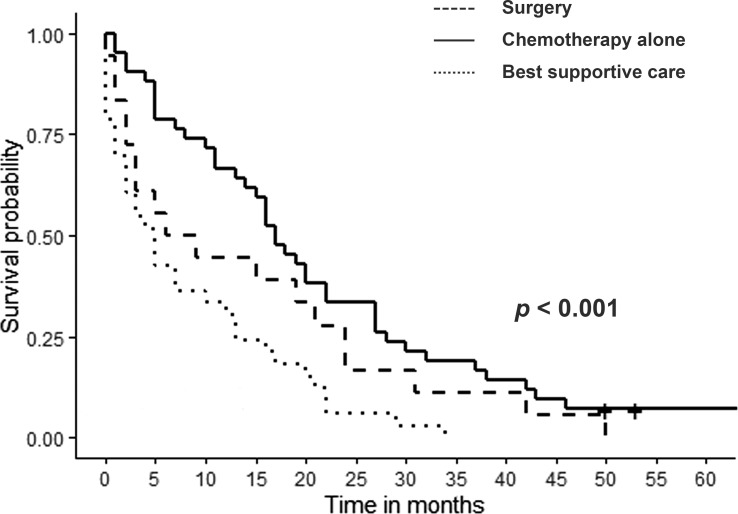
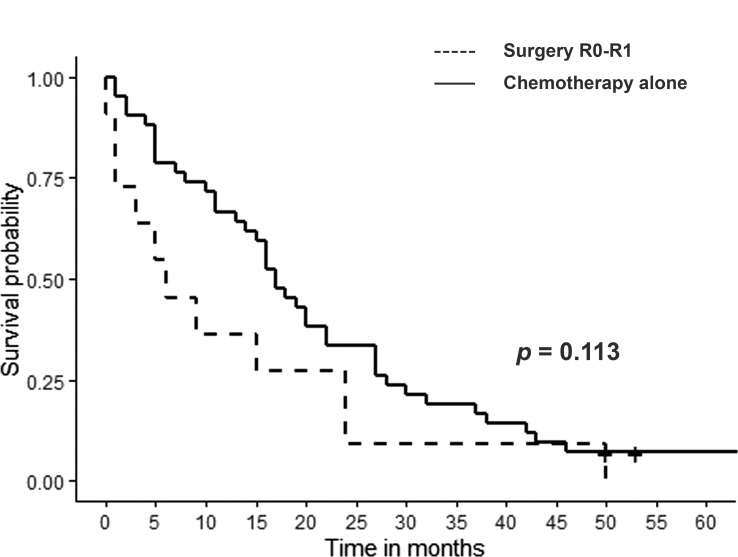
Results: Eighteen patients were indicated surgery to treat CC recurrence. Severe postoperative complication rate was 27.8% with a 30-day mortality rate of 16.7%. Median survival after surgery was 15 months (range 0-50) with 1- and 3-year patient survival rates of 55.6% and 16.6%, respectively. Patient survival after surgery or CHT alone, was significantly better than receiving supportive care (p< 0.001). We found no significant difference in survival when comparing CHT alone and surgical treatment (p=0.113). Time to recurrence of <1 year, adjuvant CHT after resection of the primary tumor and undergoing surgery or CHT alone versus best supportive care were independent factors affecting mortality after CC recurrence in the multivariate analysis.
Conclusion: Surgery or CHT alone improved patient survival after CC recurrence compared to best supportive care. Surgical treatment did not improve patient survival compared to CHT alone.
Keywords: chemotherapy; cholangiocarcinoma; outcomes; recurrence; surgical treatment.
Copyright © 2023 Fernández, Gastaca, Alonso, Prieto, Ruiz, Ventoso, Palomares, Perfecto and Valdivieso.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources