

Osteoblast-intrinsic defect in glucose metabolism impairs bone formation in type II diabetic male mice
- PMID: 37144869
- PMCID: PMC10198725
- DOI: 10.7554/eLife.85714
Osteoblast-intrinsic defect in glucose metabolism impairs bone formation in type II diabetic male mice
Abstract
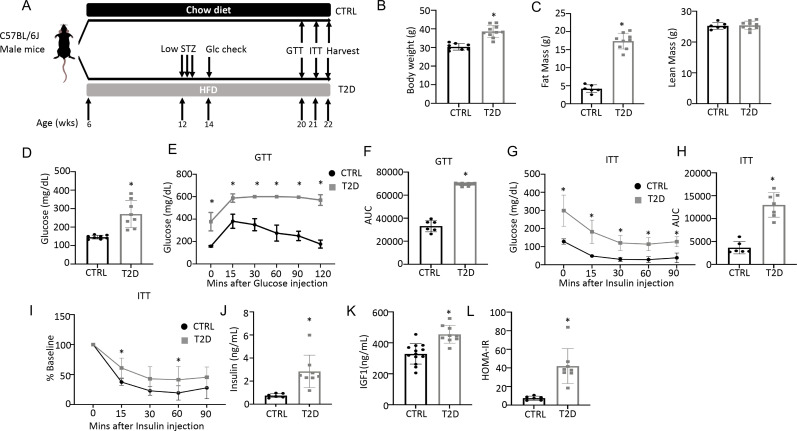
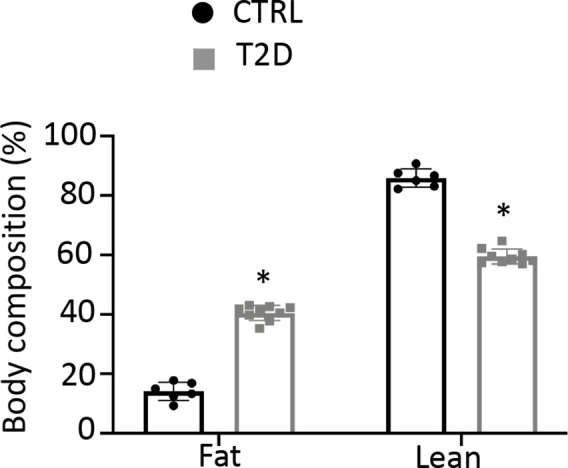
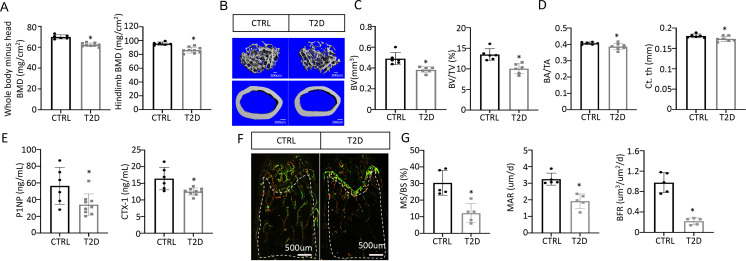
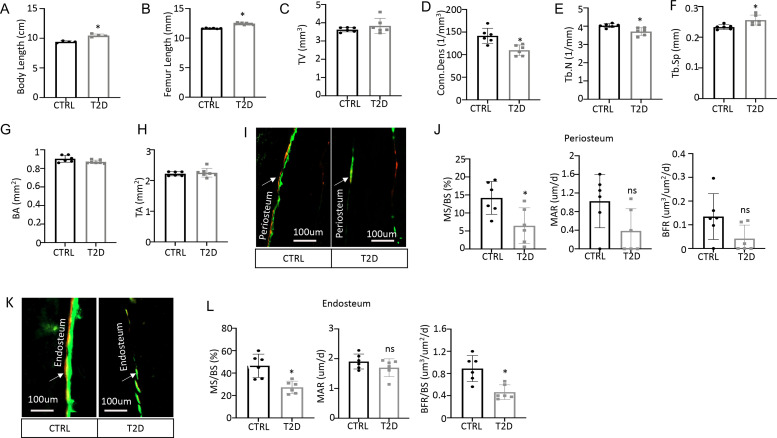
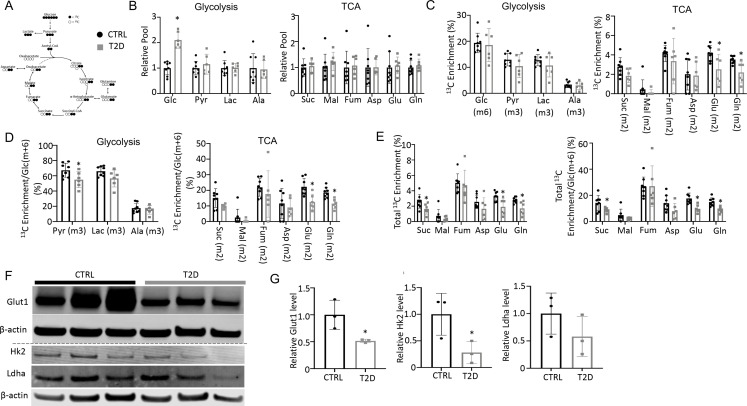
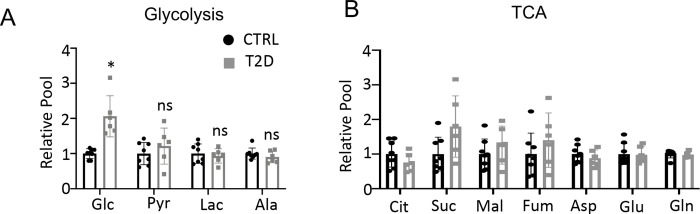
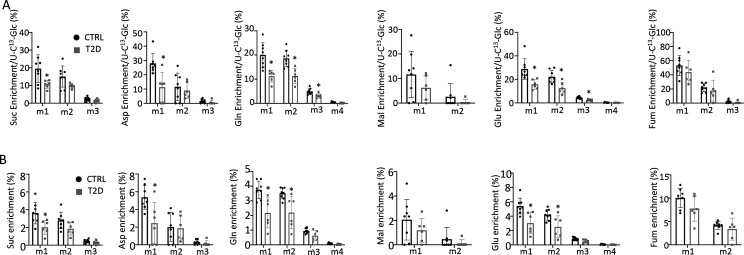
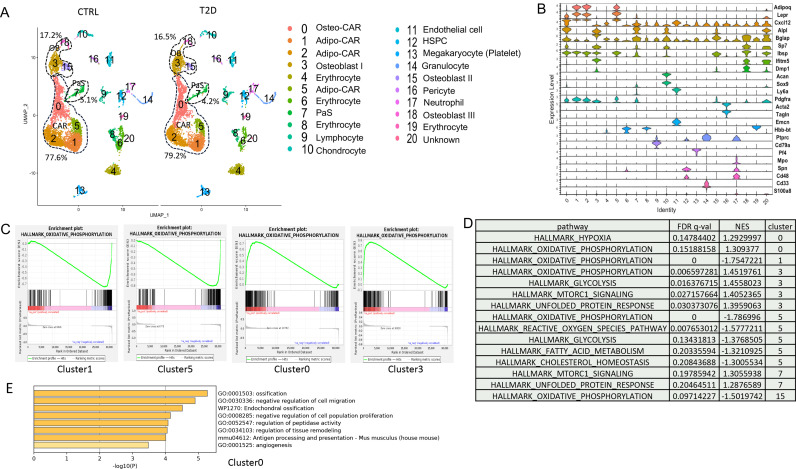
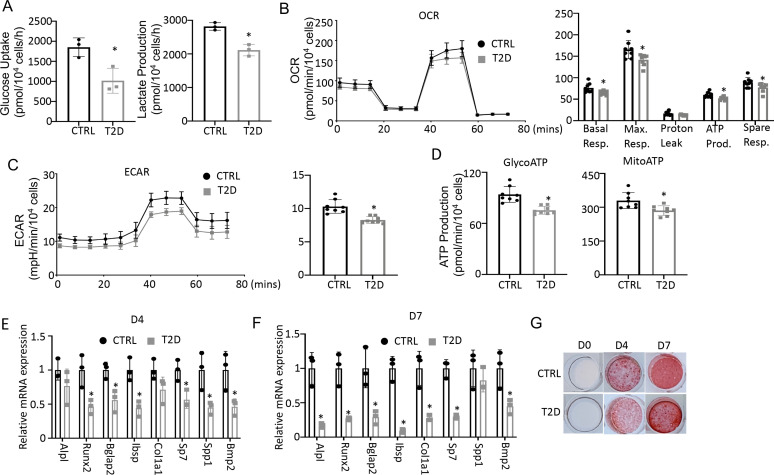
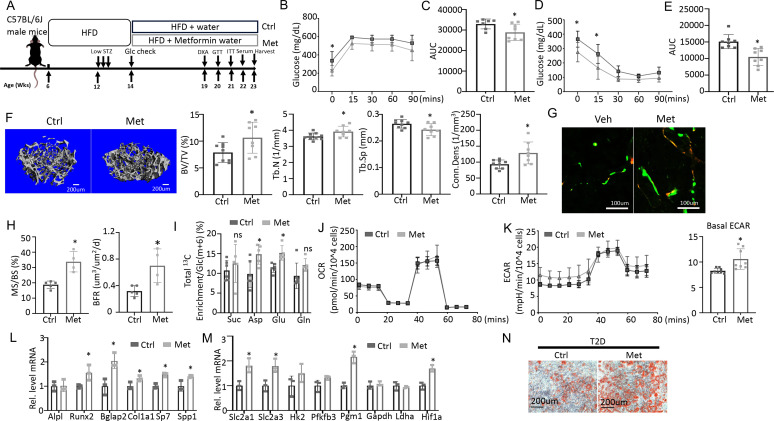
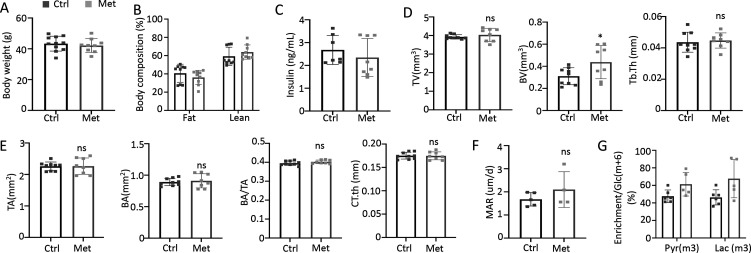
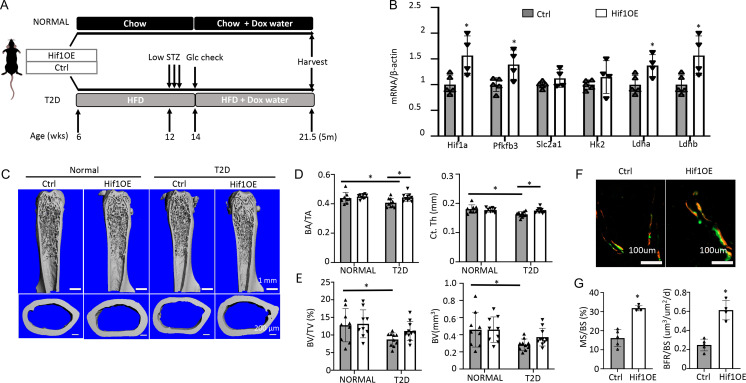
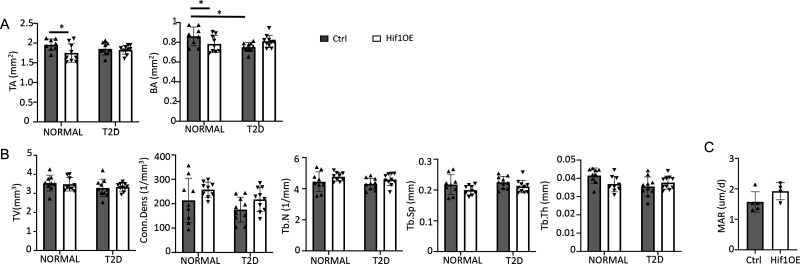
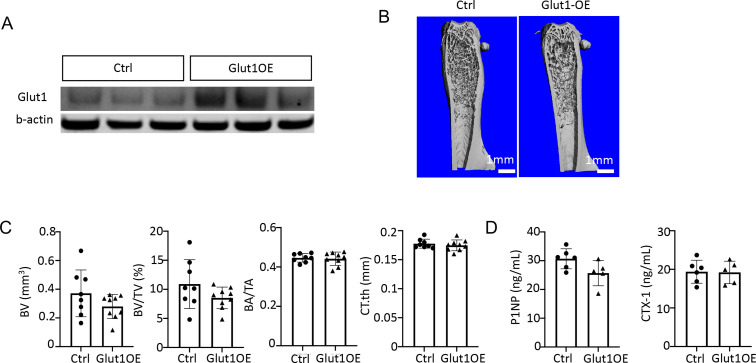
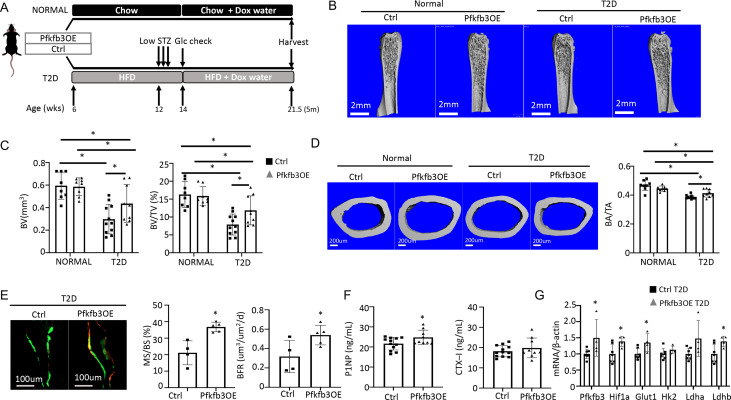
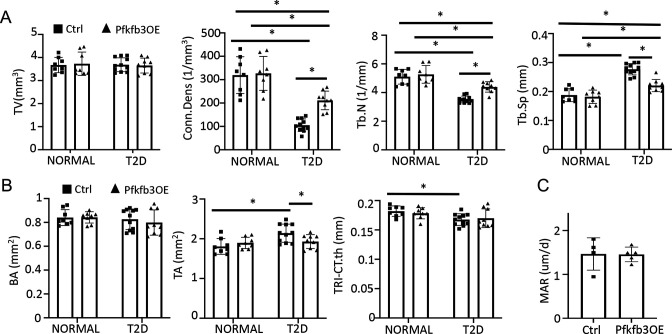
Skeletal fragility is associated with type 2 diabetes mellitus (T2D), but the underlying mechanism is not well understood. Here, in a mouse model for youth-onset T2D, we show that both trabecular and cortical bone mass is reduced due to diminished osteoblast activity. Stable isotope tracing in vivo with 13C-glucose demonstrates that both glycolysis and glucose fueling of the TCA cycle are impaired in diabetic bones. Similarly, Seahorse assays show suppression of both glycolysis and oxidative phosphorylation by diabetes in bone marrow mesenchymal cells as a whole, whereas single-cell RNA sequencing reveals distinct modes of metabolic dysregulation among the subpopulations. Metformin not only promotes glycolysis and osteoblast differentiation in vitro, but also improves bone mass in diabetic mice. Finally, osteoblast-specific overexpression of either Hif1a, a general inducer of glycolysis, or Pfkfb3 which stimulates a specific step in glycolysis, averts bone loss in T2D mice. The study identifies osteoblast-intrinsic defects in glucose metabolism as an underlying cause of diabetic osteopenia, which may be targeted therapeutically.
Keywords: bone; diabetic osteopenia; glucose metabolism; medicine; mouse; osteoblast; type II diabetes.
© 2023, Song et al.
Conflict of interest statement
FS, WL, TM, XJ, CS, XL, RS, LY, HL, FL No competing interests declared
Figures

Update of
-
Osteoblast-intrinsic defect in glucose metabolism impairs bone formation in type II diabetic mice.bioRxiv [Preprint]. 2023 Jan 18:2023.01.16.524248. doi: 10.1101/2023.01.16.524248. bioRxiv. 2023. Update in: Elife. 2023 May 05;12:e85714. doi: 10.7554/eLife.85714. PMID: 36711657 Free PMC article. Updated. Preprint.
References
-
- Baccin C, Al-Sabah J, Velten L, Helbling PM, Grünschläger F, Hernández-Malmierca P, Nombela-Arrieta C, Steinmetz LM, Trumpp A, Haas S. Combined single-cell and spatial transcriptomics reveal the molecular, cellular and spatial bone marrow niche organization. Nature Cell Biology. 2020;22:38–48. doi: 10.1038/s41556-019-0439-6. - DOI - PMC - PubMed
-
- Baryawno N, Przybylski D, Kowalczyk MS, Kfoury Y, Severe N, Gustafsson K, Kokkaliaris KD, Mercier F, Tabaka M, Hofree M, Dionne D, Papazian A, Lee D, Ashenberg O, Subramanian A, Vaishnav ED, Rozenblatt-Rosen O, Regev A, Scadden DT. A cellular taxonomy of the bone marrow stroma in homeostasis and leukemia. Cell. 2019;177:1915–1932. doi: 10.1016/j.cell.2019.04.040. - DOI - PMC - PubMed
-
- Bonds DE, Larson JC, Schwartz AV, Strotmeyer ES, Robbins J, Rodriguez BL, Johnson KC, Margolis KL. Risk of fracture in women with type 2 diabetes: the women’s health Initiative observational study. The Journal of Clinical Endocrinology and Metabolism. 2006;91:3404–3410. doi: 10.1210/jc.2006-0614. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
- Actions
- Dryad/10.5061/dryad.s7h44j1bc
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
