

Rectal cancer lexicon 2023 revised and updated consensus statement from the Society of Abdominal Radiology Colorectal and Anal Cancer Disease-Focused Panel
- PMID: 37145311
- PMCID: PMC10444656
- DOI: 10.1007/s00261-023-03893-2
Rectal cancer lexicon 2023 revised and updated consensus statement from the Society of Abdominal Radiology Colorectal and Anal Cancer Disease-Focused Panel
Abstract
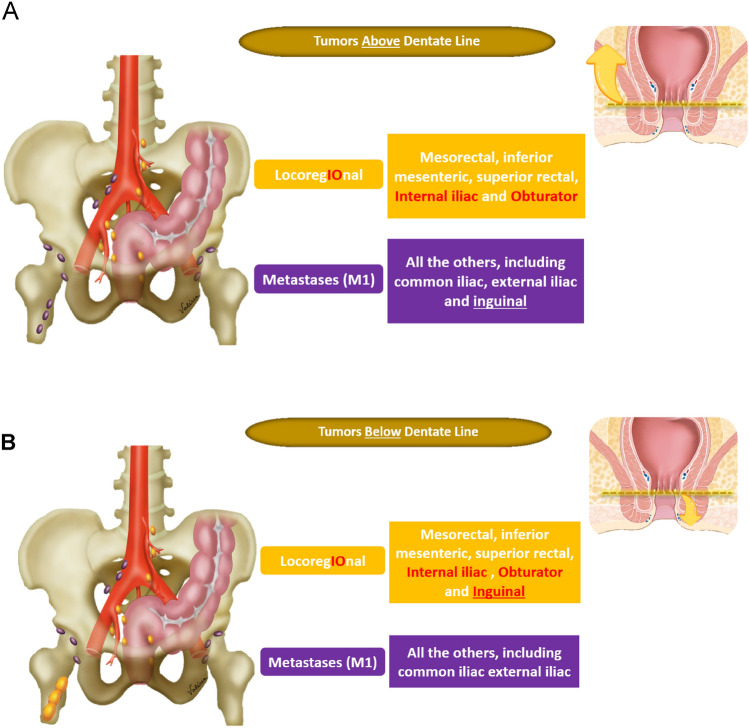
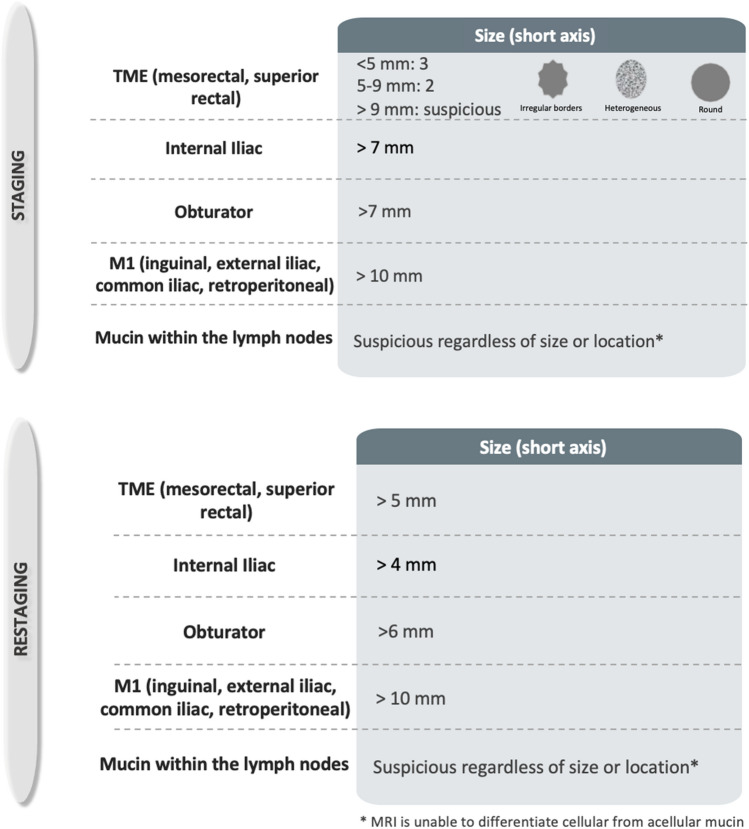
The Society of Abdominal Radiology's Colorectal and Anal Cancer Disease-Focused Panel (DFP) first published a rectal cancer lexicon paper in 2019. Since that time, the DFP has published revised initial staging and restaging reporting templates, and a new SAR user guide to accompany the rectal MRI synoptic report (primary staging). This lexicon update summarizes interval developments, while conforming to the original lexicon 2019 format. Emphasis is placed on primary staging, treatment response, anatomic terminology, nodal staging, and the utility of specific sequences in the MRI protocol. A discussion of primary tumor staging reviews updates on tumor morphology and its clinical significance, T1 and T3 subclassifications and their clinical implications, T4a and T4b imaging findings/definitions, terminology updates on the use of MRF over CRM, and the conundrum of the external sphincter. A parallel section on treatment response reviews the clinical significance of near-complete response and introduces the lexicon of "regrowth" versus "recurrence". A review of relevant anatomy incorporates updated definitions and expert consensus of anatomic landmarks, including the NCCN's new definition of rectal upper margin and sigmoid take-off. A detailed review of nodal staging is also included, with attention to tumor location relative to the dentate line and locoregional lymph node designation, a new suggested size threshold for lateral lymph nodes and their indications for use, and imaging criteria used to differentiate tumor deposits from lymph nodes. Finally, new treatment terminologies such as organ preservation, TNT, TAMIS and watch-and-wait management are introduced. This 2023 version aims to serve as a concise set of up-to-date recommendations for radiologists, and discusses terminology, classification systems, MRI and clinical staging, and the evolving concepts in diagnosis and treatment of rectal cancer.
Keywords: Gastrointestinal tract; MRI; Oncology; Rectal adenocarcinoma; Rectal cancer.
© 2023. This is a U.S. Government work and not under copyright protection in the US; foreign copyright protection may apply.
Conflict of interest statement
The authors disclose no conflict of interest.
Figures
Comment in
-
Letter to the Editor regarding the article "Rectal cancer lexicon 2023 revised and updated consensus statement from the Society of Abdominal Radiology Colorectal and Anal Cancer Disease‑Focused Panel" by Sonia Lee et al.Abdom Radiol (NY). 2023 Dec;48(12):3774-3775. doi: 10.1007/s00261-023-04057-y. Epub 2023 Sep 20. Abdom Radiol (NY). 2023. PMID: 37731067 No abstract available.
References
-
- Kassam Z, Lang R, Arya S, Bates DDB, Chang KJ, Fraum TJ, et al. Update to the structured MRI report for primary staging of rectal cancer : Perspective from the SAR Disease Focused Panel on Rectal and Anal Cancer. Abdom Radiol (NY). 2022;47(10):3364–3374. doi: 10.1007/s00261-022-03612-3. - DOI - PubMed
-
- Pimentel-Nunes P, Libanio D, Bastiaansen BAJ, Bhandari P, Bisschops R, Bourke MJ, et al. Endoscopic submucosal dissection for superficial gastrointestinal lesions: European Society of Gastrointestinal Endoscopy (ESGE) Guideline - Update 2022. Endoscopy. 2022;54(6):591–622. doi: 10.1055/a-1811-7025. - DOI - PubMed
-
- Kikuchi R, Takano M, Takagi K, Fujimoto N, Nozaki R, Fujiyoshi T, et al. Management of early invasive colorectal cancer. Risk of recurrence and clinical guidelines. Dis Colon Rectum. 1995;38(12):1286–95. doi: 10.1007/BF02049154. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
