

Cytokinopathy with aberrant cytotoxic lymphocytes and profibrotic myeloid response in SARS-CoV-2 mRNA vaccine-associated myocarditis
- PMID: 37146127
- PMCID: PMC10468758
- DOI: 10.1126/sciimmunol.adh3455
Cytokinopathy with aberrant cytotoxic lymphocytes and profibrotic myeloid response in SARS-CoV-2 mRNA vaccine-associated myocarditis
Abstract
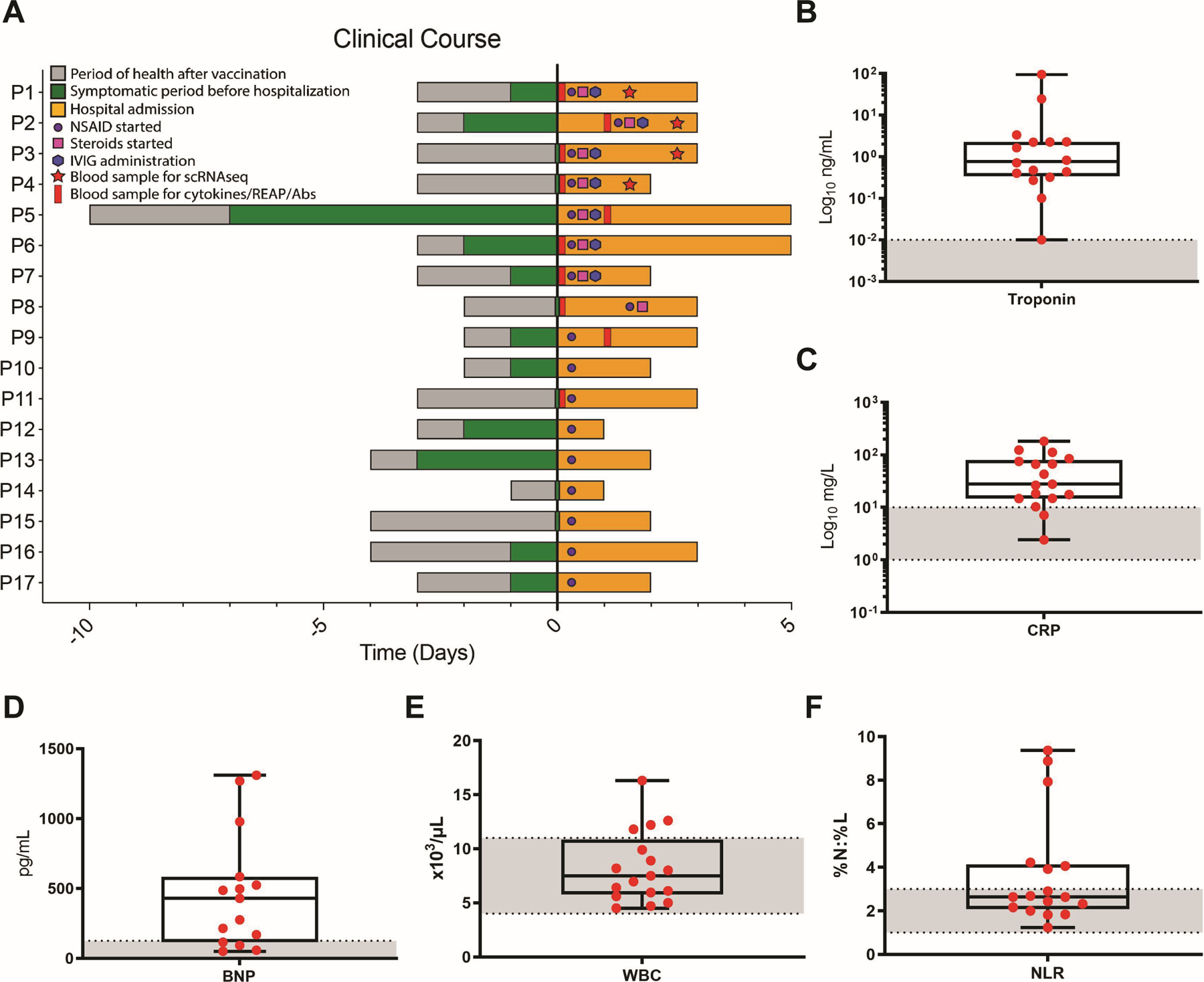
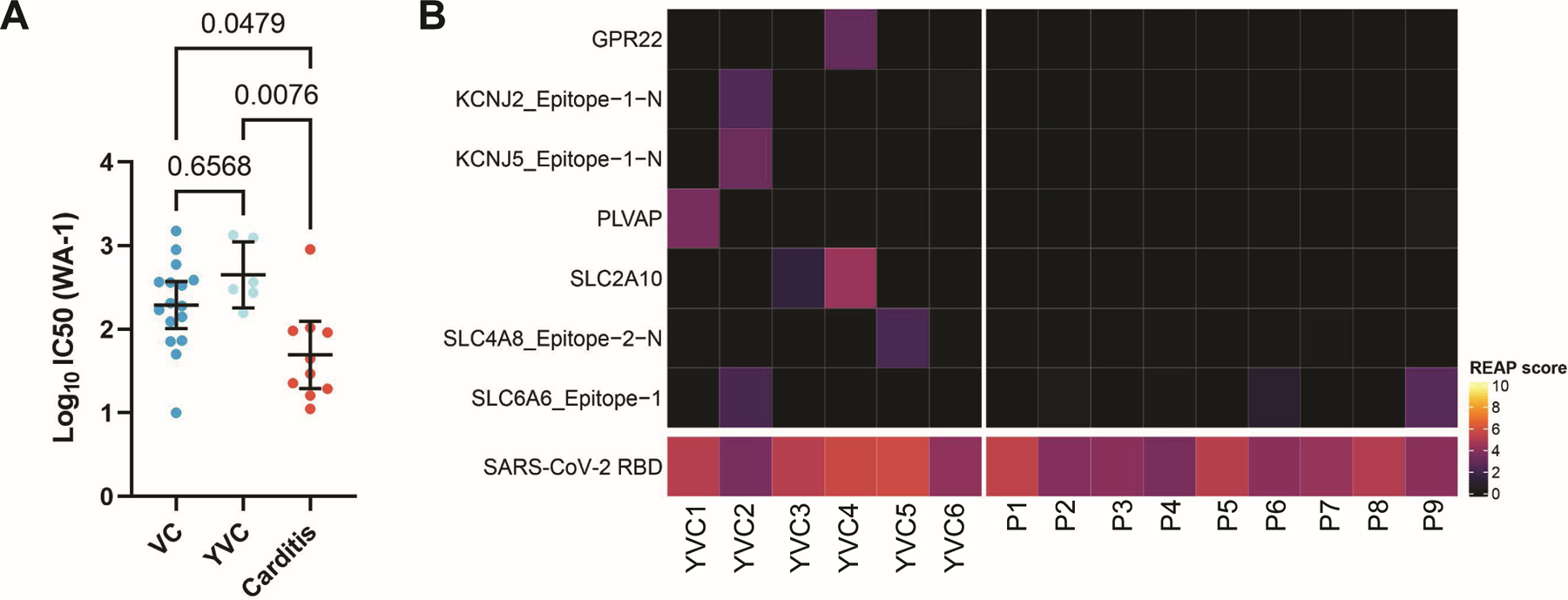
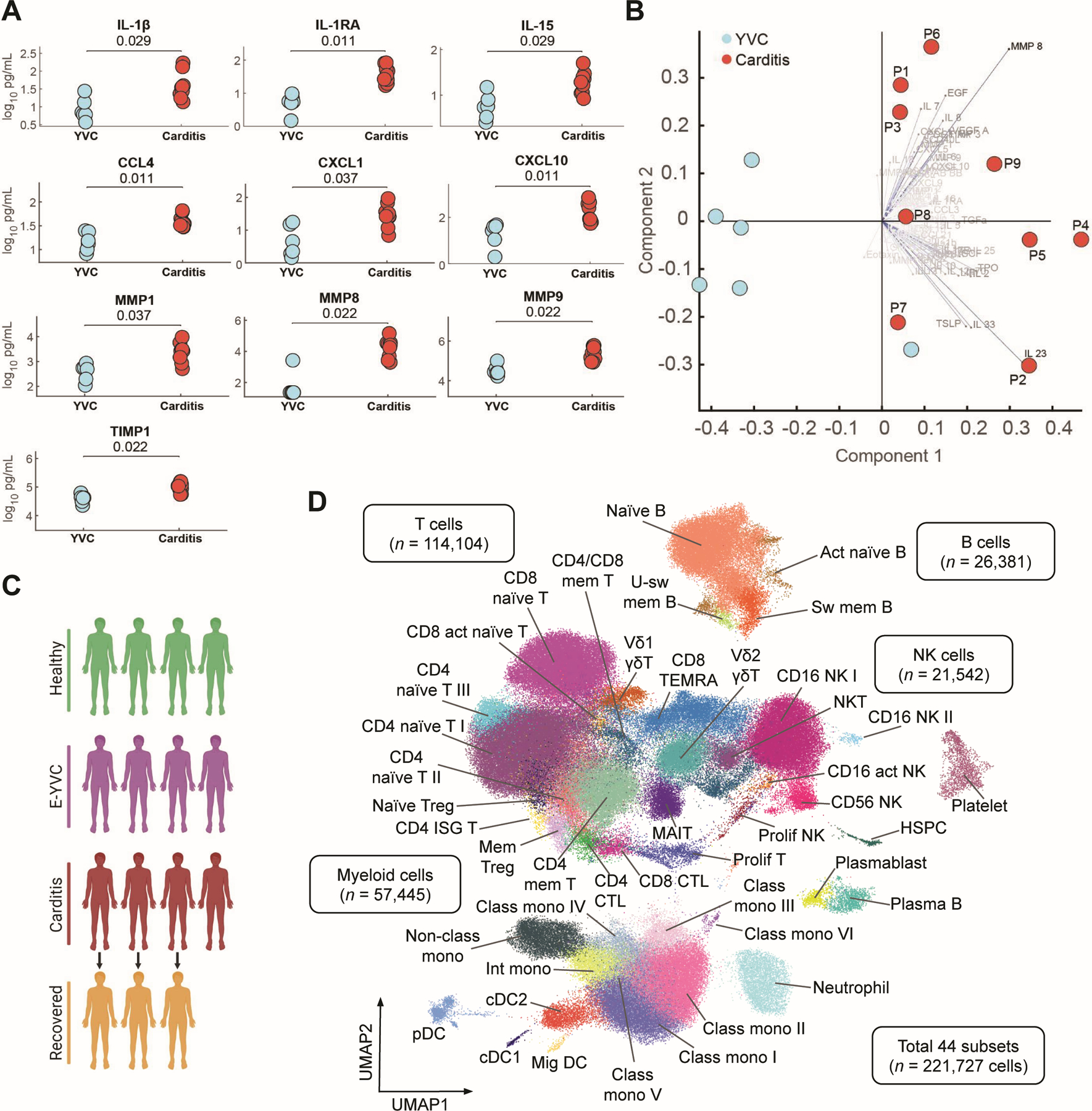
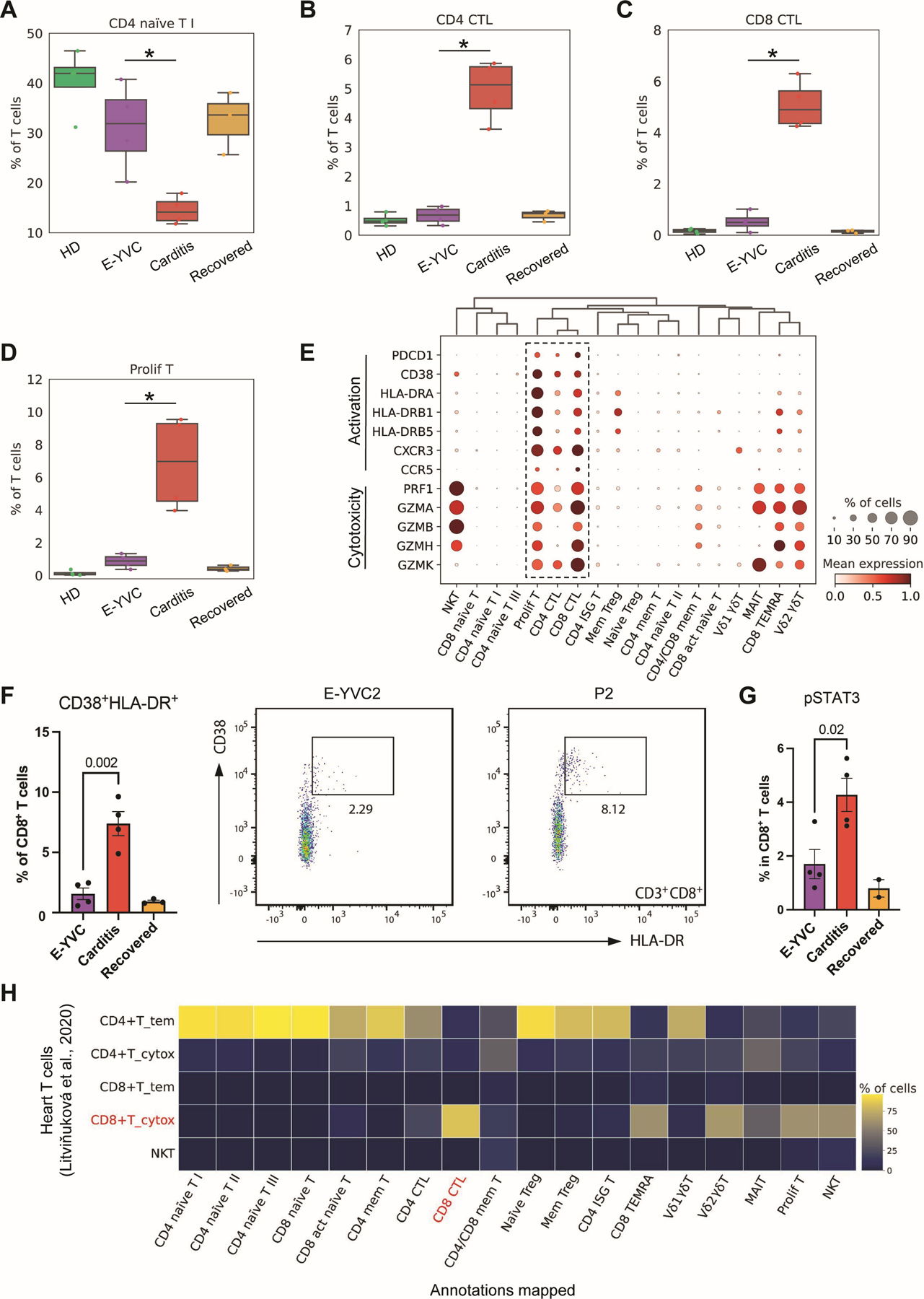
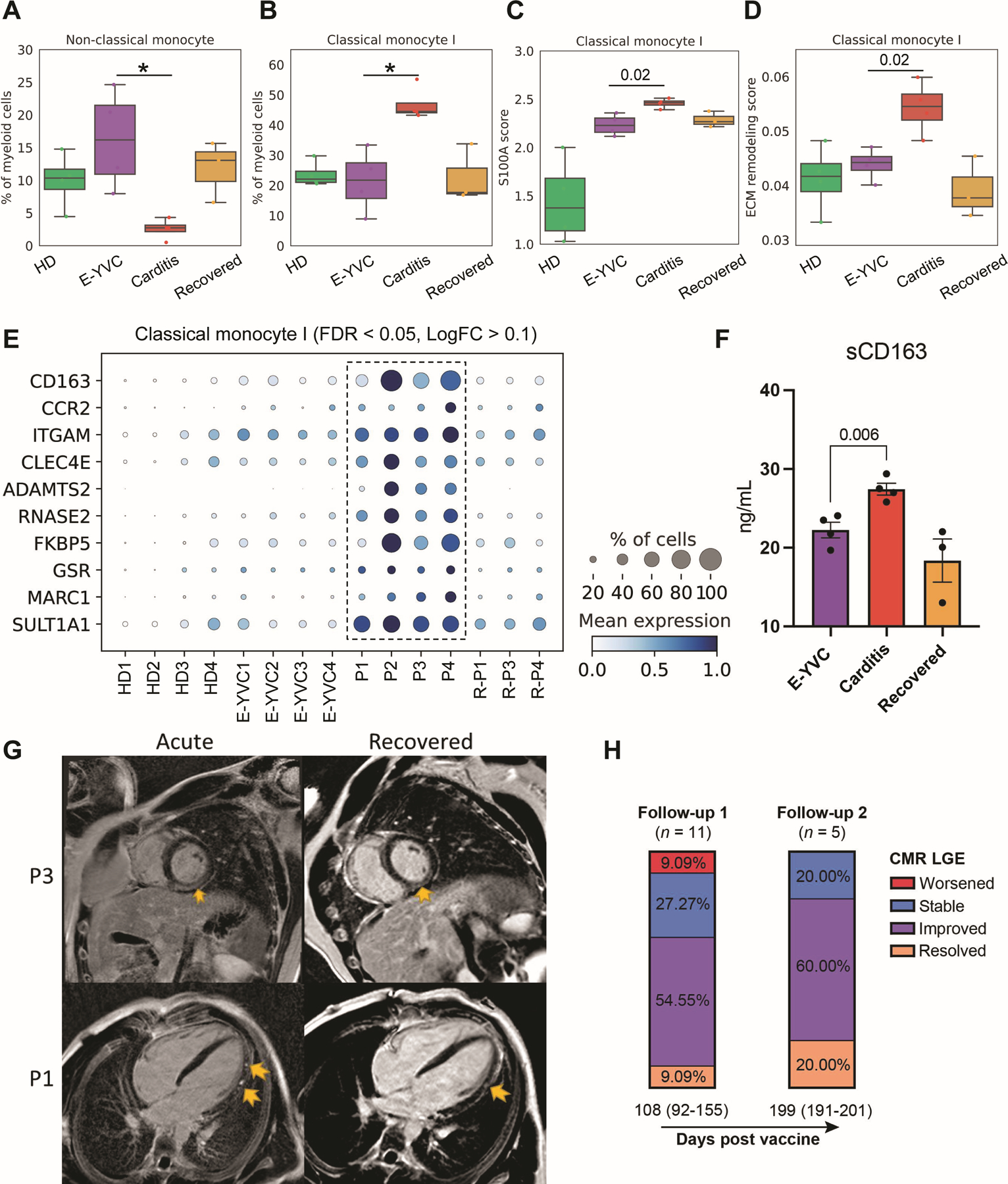
Rare immune-mediated cardiac tissue inflammation can occur after vaccination, including after SARS-CoV-2 mRNA vaccines. However, the underlying immune cellular and molecular mechanisms driving this pathology remain poorly understood. Here, we investigated a cohort of patients who developed myocarditis and/or pericarditis with elevated troponin, B-type natriuretic peptide, and C-reactive protein levels as well as cardiac imaging abnormalities shortly after SARS-CoV-2 mRNA vaccination. Contrary to early hypotheses, patients did not demonstrate features of hypersensitivity myocarditis, nor did they have exaggerated SARS-CoV-2-specific or neutralizing antibody responses consistent with a hyperimmune humoral mechanism. We additionally found no evidence of cardiac-targeted autoantibodies. Instead, unbiased systematic immune serum profiling revealed elevations in circulating interleukins (IL-1β, IL-1RA, and IL-15), chemokines (CCL4, CXCL1, and CXCL10), and matrix metalloproteases (MMP1, MMP8, MMP9, and TIMP1). Subsequent deep immune profiling using single-cell RNA and repertoire sequencing of peripheral blood mononuclear cells during acute disease revealed expansion of activated CXCR3+ cytotoxic T cells and NK cells, both phenotypically resembling cytokine-driven killer cells. In addition, patients displayed signatures of inflammatory and profibrotic CCR2+ CD163+ monocytes, coupled with elevated serum-soluble CD163, that may be linked to the late gadolinium enhancement on cardiac MRI, which can persist for months after vaccination. Together, our results demonstrate up-regulation in inflammatory cytokines and corresponding lymphocytes with tissue-damaging capabilities, suggesting a cytokine-dependent pathology, which may further be accompanied by myeloid cell-associated cardiac fibrosis. These findings likely rule out some previously proposed mechanisms of mRNA vaccine--associated myopericarditis and point to new ones with relevance to vaccine development and clinical care.
Conflict of interest statement
Figures
Comment in
-
Cytokinopathy drives SARS-CoV-2 vaccination-associated myopericarditis.Nat Cardiovasc Res. 2023 Jun;2(6):489. doi: 10.1038/s44161-023-00290-2. Nat Cardiovasc Res. 2023. PMID: 39195883 No abstract available.
References
-
- Baden LR, El Sahly HM, Essink B, Kotloff K, Frey S, Novak R, Diemert D, Spector SA, Rouphael N, Creech CB, McGettigan J, Khetan S, Segall N, Solis J, Brosz A, Fierro C, Schwartz H, Neuzil K, Corey L, Gilbert P, Janes H, Follmann D, Marovich M, Mascola J, Polakowski L, Ledgerwood J, Graham BS, Bennett H, Pajon R, Knightly C, Leav B, Deng W, Zhou H, Han S, Ivarsson M, Miller J, Zaks T, Group CS. 2021. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N Engl J Med 384: 403–16 - PMC - PubMed
-
- Polack FP, Thomas SJ, Kitchin N, Absalon J, Gurtman A, Lockhart S, Perez JL, Perez Marc G, Moreira ED, Zerbini C, Bailey R, Swanson KA, Roychoudhury S, Koury K, Li P, Kalina WV, Cooper D, Frenck RW Jr., Hammitt LL, Tureci O, Nell H, Schaefer A, Unal S, Tresnan DB, Mather S, Dormitzer PR, Sahin U, Jansen KU, Gruber WC, Group CCT. 2020. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N Engl J Med 383: 2603–15 - PMC - PubMed
-
- Shimabukuro TT, Kim SY, Myers TR, Moro PL, Oduyebo T, Panagiotakopoulos L, Marquez PL, Olson CK, Liu R, Chang KT, Ellington SR, Burkel VK, Smoots AN, Green CJ, Licata C, Zhang BC, Alimchandani M, Mba-Jonas A, Martin SW, Gee JM, Meaney-Delman DM, Team CDCv-sC-PR. 2021. Preliminary Findings of mRNA Covid-19 Vaccine Safety in Pregnant Persons. N Engl J Med 384: 2273–82 - PMC - PubMed
-
- Patone M, Mei XW, Handunnetthi L, Dixon S, Zaccardi F, Shankar-Hari M, Watkinson P, Khunti K, Harnden A, Coupland CAC, Channon KM, Mills NL, Sheikh A, Hippisley-Cox J. 2021. Risks of myocarditis, pericarditis, and cardiac arrhythmias associated with COVID-19 vaccination or SARS-CoV-2 infection. Nature Medicine - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
