

Deep Phenotyping of Neurologic Postacute Sequelae of SARS-CoV-2 Infection
- PMID: 37147136
- PMCID: PMC10162706
- DOI: 10.1212/NXI.0000000000200097
Deep Phenotyping of Neurologic Postacute Sequelae of SARS-CoV-2 Infection
Abstract
Background and objectives: SARS-CoV-2 infection has been associated with a syndrome of long-term neurologic sequelae that is poorly characterized. We aimed to describe and characterize in-depth features of neurologic postacute sequelae of SARS-CoV-2 infection (neuro-PASC).
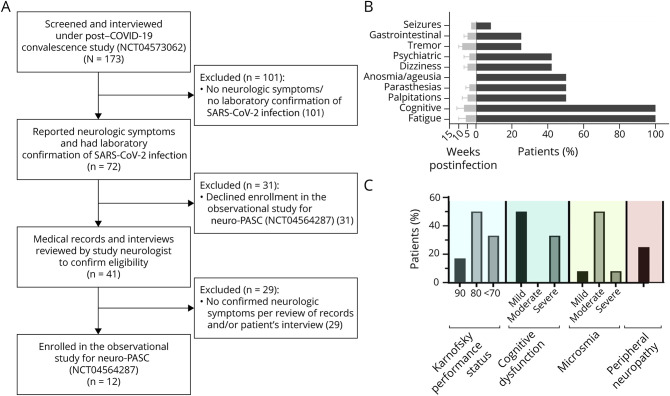
Methods: Between October 2020 and April 2021, 12 participants were seen at the NIH Clinical Center under an observational study to characterize ongoing neurologic abnormalities after SARS-CoV-2 infection. Autonomic function and CSF immunophenotypic analysis were compared with healthy volunteers (HVs) without prior SARS-CoV-2 infection tested using the same methodology.
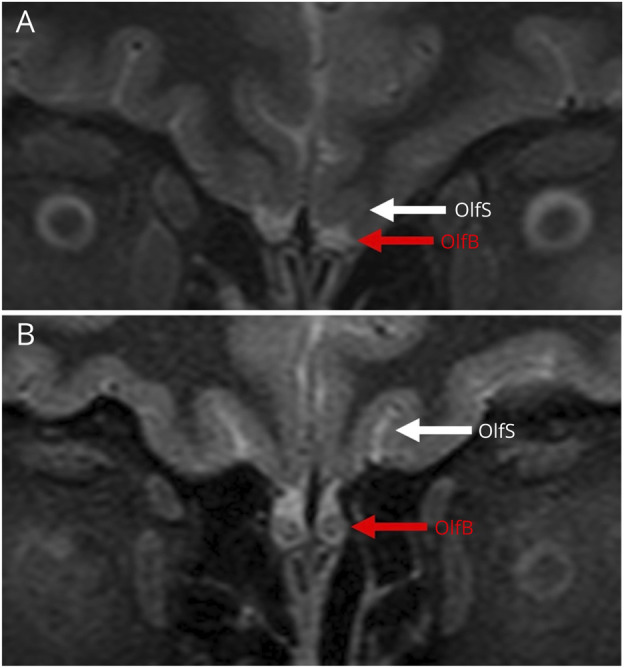
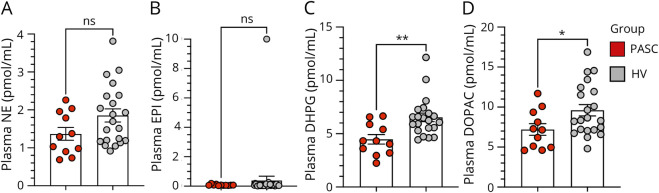
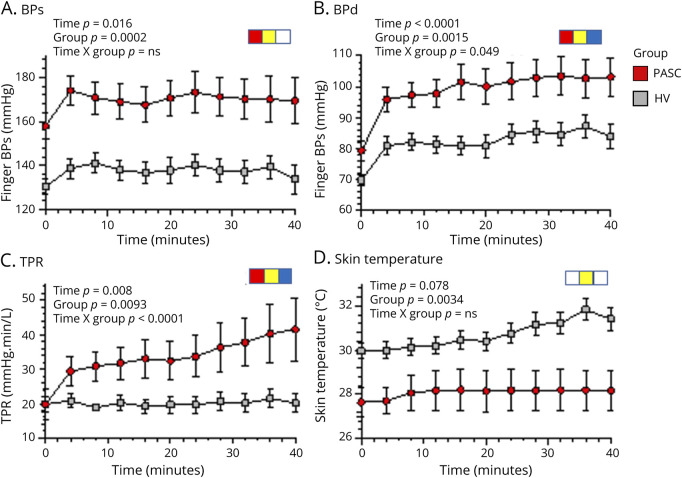
Results: Participants were mostly female (83%), with a mean age of 45 ± 11 years. The median time of evaluation was 9 months after COVID-19 (range 3-12 months), and most (11/12, 92%) had a history of only a mild infection. The most common neuro-PASC symptoms were cognitive difficulties and fatigue, and there was evidence for mild cognitive impairment in half of the patients (MoCA score <26). The majority (83%) had a very disabling disease, with Karnofsky Performance Status ≤80. Smell testing demonstrated different degrees of microsmia in 8 participants (66%). Brain MRI scans were normal, except 1 patient with bilateral olfactory bulb hypoplasia that was likely congenital. CSF analysis showed evidence of unique intrathecal oligoclonal bands in 3 cases (25%). Immunophenotyping of CSF compared with HVs showed that patients with neuro-PASC had lower frequencies of effector memory phenotype both for CD4+ T cells (p < 0.0001) and for CD8+ T cells (p = 0.002), an increased frequency of antibody-secreting B cells (p = 0.009), and increased frequency of cells expressing immune checkpoint molecules. On autonomic testing, there was evidence for decreased baroreflex-cardiovagal gain (p = 0.009) and an increased peripheral resistance during tilt-table testing (p < 0.0001) compared with HVs, without excessive plasma catecholamine responses.
Discussion: CSF immune dysregulation and neurocirculatory abnormalities after SARS-CoV-2 infection in the setting of disabling neuro-PASC call for further evaluation to confirm these changes and explore immunomodulatory treatments in the context of clinical trials.
Written work prepared by employees of the Federal Government as part of their official duties is, under the U.S. Copyright Act, a “work of the United States Government” for which copyright protection under Title 17 of the United States Code is not available. As such, copyright does not extend to the contributions of employees of the Federal Government.
Conflict of interest statement
The authors report no disclosures relevant to the manuscript. Go to
Figures


References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous