

Pancreatic duct imaging during aging
- PMID: 37148134
- PMCID: PMC10237600
- DOI: 10.4103/EUS-D-22-00119
Pancreatic duct imaging during aging
Abstract
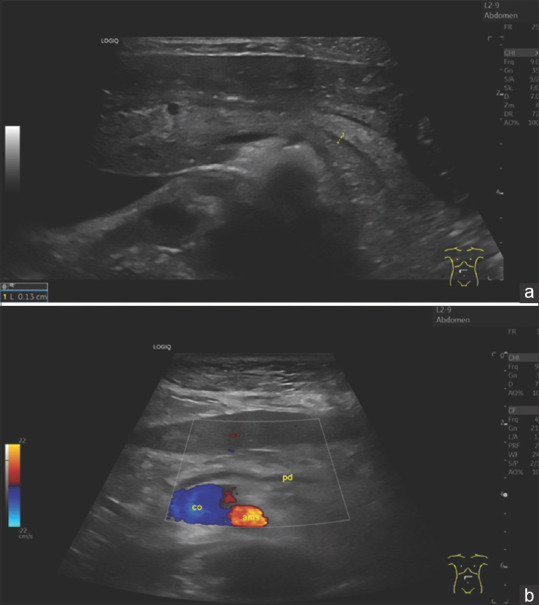
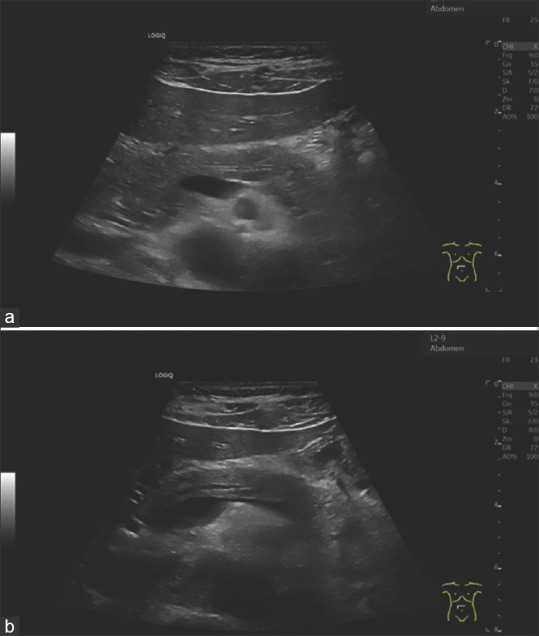
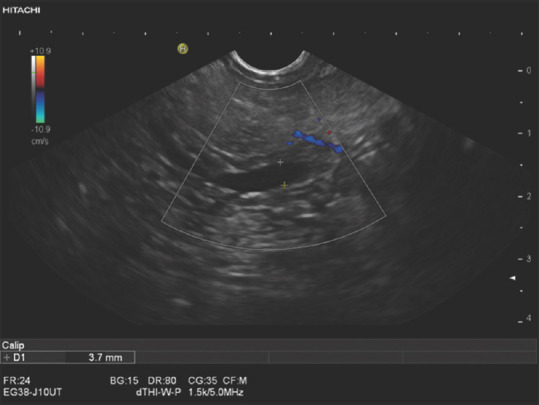
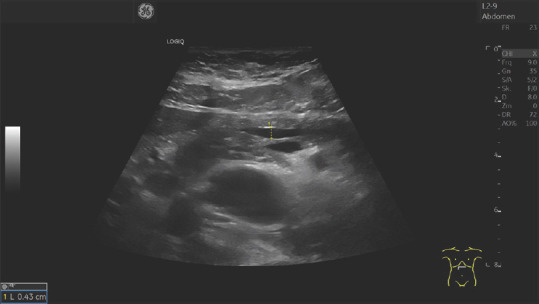
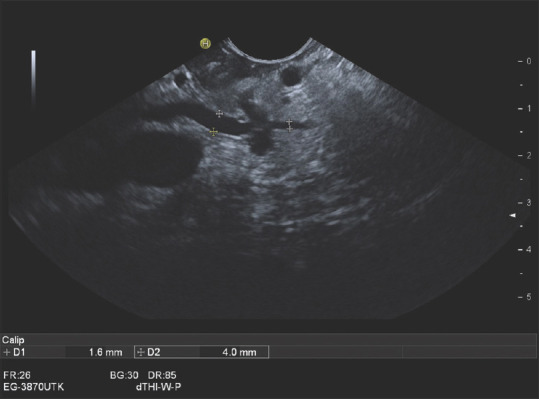
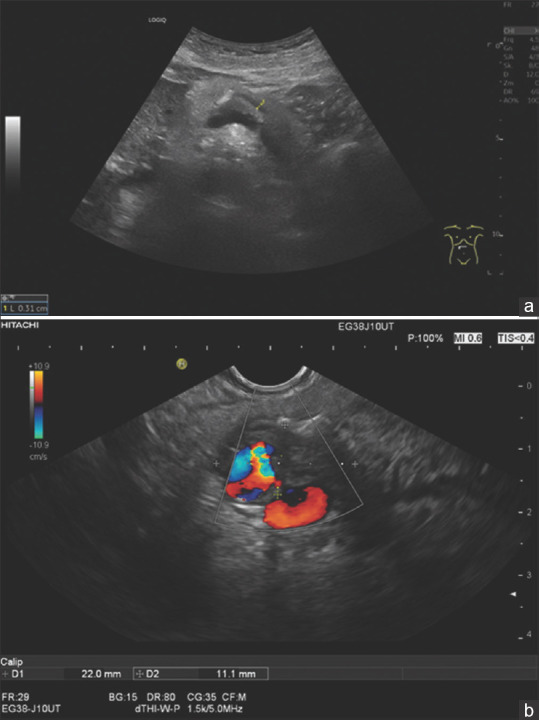
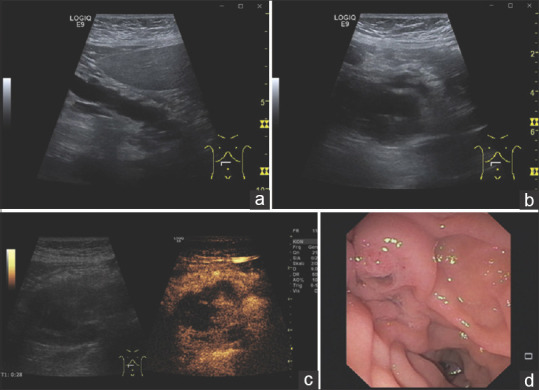
As part of the aging process, fibrotic changes, fatty infiltration, and parenchymal atrophy develop in the pancreas. The pancreatic duct also becomes wider with age. This article provides an overview of the diameter of the pancreatic duct in different age groups and different examination methods. Knowledge of these data is useful to avoid misinterpretations regarding the differential diagnosis of chronic pancreatitis, obstructive tumors, and intraductal papillary mucinous neoplasia (IPMN).
Keywords: EUS; aging; diameter; ductal adenocarcinoma; pancreatic duct.
Conflict of interest statement
Siyu Sun is the Editor-in-Chief of the journal; Christoph F. Dietrich is a Co-Editor-in-Chief; Christian Jenssen, Michael Hocke and Julio Iglesias-Garcia are Editorial Board Members. This article was subject to the journal’s standard procedures, with peer review handled independently of the editors and their research groups.
Figures
References
-
- United Nations. World Population Ageing 2019:Highlights. New York: United Nations; 2019.
-
- Löhr JM, Panic N, Vujasinovic M, et al. The ageing pancreas:A systematic review of the evidence and analysis of the consequences. J Intern Med. 2018;283:446–60. - PubMed
-
- Stamm BH. Incidence and diagnostic significance of minor pathologic changes in the adult pancreas at autopsy:A systematic study of 112 autopsies in patients without known pancreatic disease. Hum Pathol. 1984;15:677–83. - PubMed
-
- Olsen TS. Lipomatosis of the pancreas in autopsy material and its relation to age and overweight. Acta Pathol Microbiol Scand A. 1978;86:367–73. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
