

Intracranial injection of natural killer cells engineered with a HER2-targeted chimeric antigen receptor in patients with recurrent glioblastoma
- PMID: 37148198
- PMCID: PMC10628939
- DOI: 10.1093/neuonc/noad087
Intracranial injection of natural killer cells engineered with a HER2-targeted chimeric antigen receptor in patients with recurrent glioblastoma
Abstract
Background: Glioblastoma (GB) is incurable at present without established treatment options for recurrent disease. In this phase I first-in-human clinical trial we investigated safety and feasibility of adoptive transfer of clonal chimeric antigen receptor (CAR)-NK cells (NK-92/5.28.z) targeting HER2, which is expressed at elevated levels by a subset of glioblastomas.
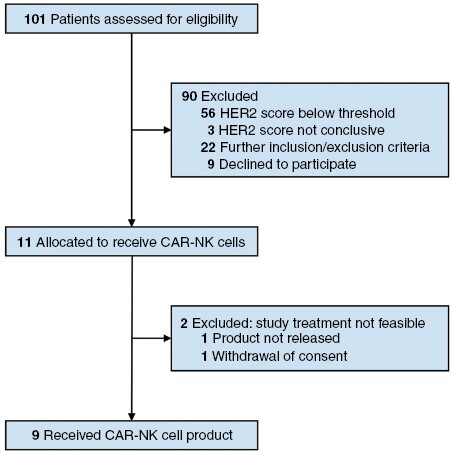
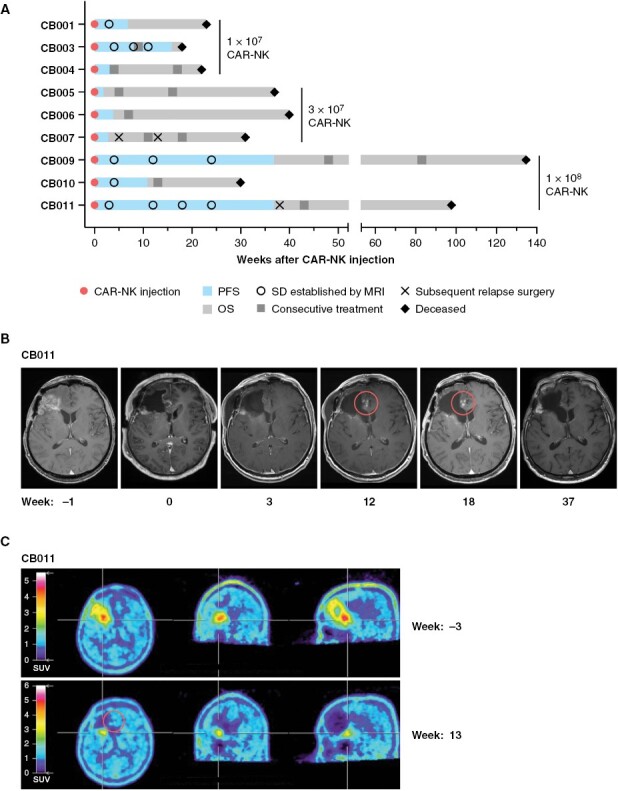
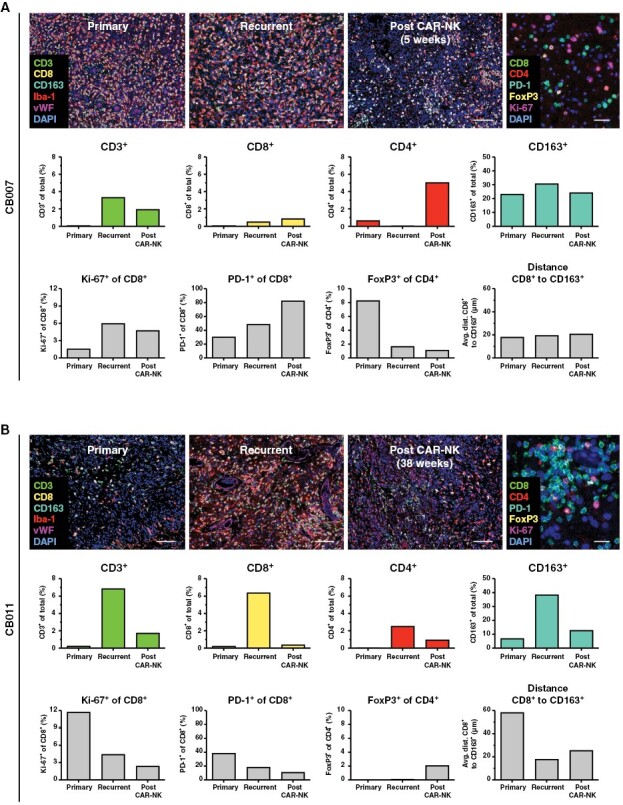
Methods: Nine patients with recurrent HER2-positive GB were treated with single doses of 1 × 107, 3 × 107, or 1 × 108 irradiated CAR-NK cells injected into the margins of the surgical cavity during relapse surgery. Imaging at baseline and follow-up, peripheral blood lymphocyte phenotyping and analyses of the immune architecture by multiplex immunohistochemistry and spatial digital profiling were performed.
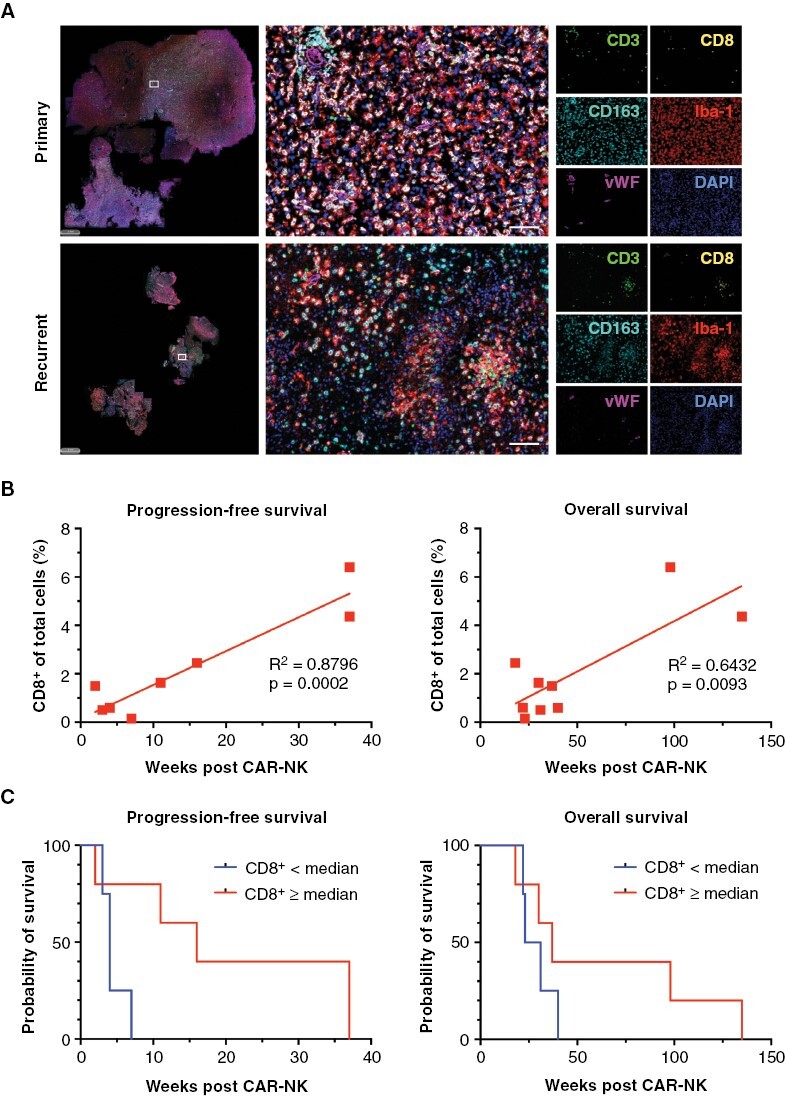
Results: There were no dose-limiting toxicities, and none of the patients developed a cytokine release syndrome or immune effector cell-associated neurotoxicity syndrome. Five patients showed stable disease after relapse surgery and CAR-NK injection that lasted 7 to 37 weeks. Four patients had progressive disease. Pseudoprogression was found at injection sites in 2 patients, suggestive of a treatment-induced immune response. For all patients, median progression-free survival was 7 weeks, and median overall survival was 31 weeks. Furthermore, the level of CD8+ T-cell infiltration in recurrent tumor tissue prior to CAR-NK cell injection positively correlated with time to progression.
Conclusions: Intracranial injection of HER2-targeted CAR-NK cells is feasible and safe in patients with recurrent GB. 1 × 108 NK-92/5.28.z cells was determined as the maximum feasible dose for a subsequent expansion cohort with repetitive local injections of CAR-NK cells.
Keywords: CAR; HER2; NK cells; adoptive immunotherapy; glioblastoma; human clinical trial; in; phase I first.
© The Author(s) 2023. Published by Oxford University Press on behalf of the Society for Neuro-Oncology.
Conflict of interest statement
CZ, TT, and WSW are named as inventors on patents and patent applications related to the study therapeutic owned by their respective academic institutions. MCB received honoraria for lectures or advisory board participation from Bristol Myers Squibb and Gilead Sciences. CS received honoraria for lectures, advisory board participation, expert testimony, or travel support from Stryker, Bayer, Brainlab, and Novocure. JPS received grants from Merck and UCB as well as honoraria for lectures, travel, or advisory board participation from Abbvie, Bristol-Myers Squibb, Medac, Roche, Novocure, and UCB. HB acknowledges speakers’ and advisory board honoraria from Boehringer-Ingelheim, Bristol Myers Squibb, Novartis, Sandoz-Hexal, and Medac as well as royalties and licensing fees from Medac, all unrelated to the work presented herein. No potential conflicts of interest were disclosed by the other authors.
Figures
Comment in
-
Chimeric antigen receptors in the brain: Can we tackle glioblastoma with engineered NK cells?Neuro Oncol. 2023 Nov 2;25(11):2072-2073. doi: 10.1093/neuonc/noad131. Neuro Oncol. 2023. PMID: 37522296 Free PMC article. No abstract available.
References
-
- Lombardi G, De Salvo GL, Brandes AA, et al. Regorafenib compared with lomustine in patients with relapsed glioblastoma (REGOMA): A multicentre, open-label, randomised, controlled, phase 2 trial. Lancet Oncol. 2019;20(1):110–119. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
