

A prospective ultrasound study of cigarette smoking and uterine leiomyomata incidence and growth
- PMID: 37148957
- PMCID: PMC10524545
- DOI: 10.1016/j.ajog.2023.04.041
A prospective ultrasound study of cigarette smoking and uterine leiomyomata incidence and growth
Abstract
Background: Uterine leiomyomata (fibroids) are common, benign neoplasms that contribute substantially to gynecologic morbidity. Some existing epidemiologic studies indicate that cigarette smoking is associated with lower uterine leiomyomata risk. However, no prospective studies have systematically screened an entire study population for uterine leiomyomata using transvaginal ultrasound or evaluated the association between cigarette smoking and uterine leiomyomata growth.
Objective: This study aimed to examine the association between cigarette smoking and uterine leiomyomata incidence and growth in a prospective ultrasound study.
Study design: We enrolled 1693 residents from the Detroit metropolitan area into the Study of Environment, Lifestyle, and Fibroids during 2010 to 2012. Eligible participants were aged 23 to 34 years, had an intact uterus but no previous diagnosis of uterine leiomyomata, and self-identified as Black or African American. We invited participants to complete a baseline visit and 4 follow-up visits over approximately 10 years. At each visit, we used transvaginal ultrasound to assess uterine leiomyomata incidence and growth. Participants provided extensive self-reported data throughout follow-up including exposures to active and passive cigarette smoking in adulthood. We excluded participants who did not return for any follow-up visits (n=76; 4%). We fit Cox proportional hazards regression models to estimate hazard ratios and 95% confidence intervals for the association between time-varying smoking history and incidence rates of uterine leiomyomata. We fit linear mixed models to estimate the percentage difference and 95% confidence intervals for the association between smoking history and uterine leiomyomata growth. We adjusted for sociodemographic, lifestyle, and reproductive factors. We interpreted our results based on magnitude and precision rather than binary significance testing.
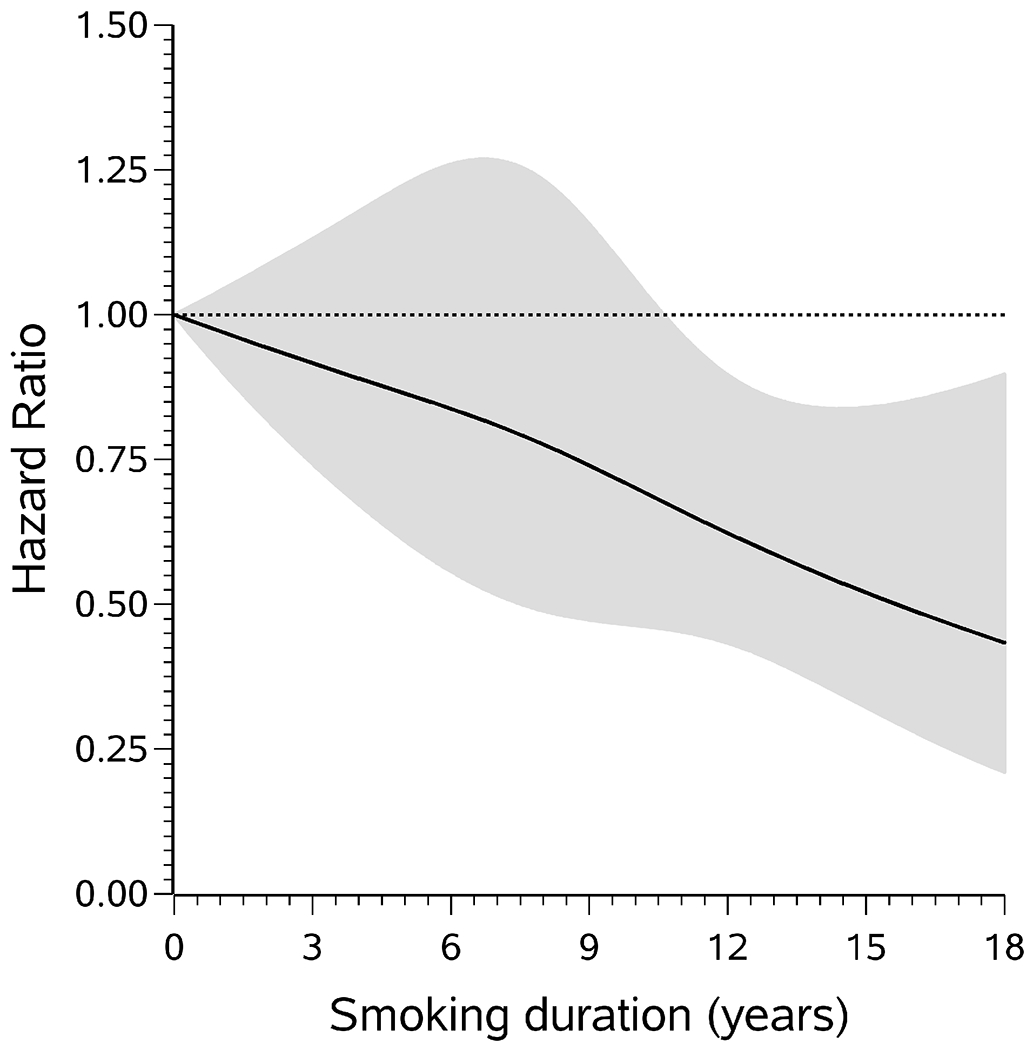
Results: Among 1252 participants without ultrasound evidence of uterine leiomyomata at baseline, uterine leiomyomata were detected in 394 participants (31%) during follow-up. Current cigarette smoking was associated with a lower uterine leiomyomata incidence rate (hazard ratio, 0.67; 95% confidence interval, 0.49-0.92). Associations were stronger among participants who had smoked for longer durations (≥15 years vs never: hazard ratio, 0.49; 95% confidence interval, 0.25-0.95). The hazard ratio for former smokers was 0.78 (95% confidence interval, 0.50-1.20). Among never smokers, the hazard ratio for current passive smoke exposure was 0.84 (95% confidence interval, 0.65-1.07). Uterine leiomyomata growth was not appreciably associated with current (percent difference, -3%; 95% confidence interval, -13% to 8%) or former (percent difference, -9%; 95% confidence interval, -22% to 6%) smoking.
Conclusion: We provide evidence from a prospective ultrasound study that cigarette smoking is associated with lower uterine leiomyomata incidence.
Keywords: cigarette smoking; fibroids; prospective cohort study; transvaginal ultrasound; uterine leiomyomata.
Copyright © 2023 Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Intake of Lycopene and other Carotenoids and Incidence of Uterine Leiomyomata: A Prospective Ultrasound Study.J Acad Nutr Diet. 2021 Jan;121(1):92-104. doi: 10.1016/j.jand.2020.08.013. Epub 2020 Oct 21. J Acad Nutr Diet. 2021. PMID: 33350944 Free PMC article.
-
Associations of per- and polyfluoroalkyl substances with uterine leiomyomata incidence and growth: a prospective ultrasound study.J Expo Sci Environ Epidemiol. 2025 May;35(3):466-477. doi: 10.1038/s41370-024-00698-3. Epub 2024 Jun 24. J Expo Sci Environ Epidemiol. 2025. PMID: 38914782
-
Urinary concentrations of phenols, parabens, and triclocarban in relation to uterine leiomyomata incidence and growth.Fertil Steril. 2021 Dec;116(6):1590-1600. doi: 10.1016/j.fertnstert.2021.07.003. Epub 2021 Aug 5. Fertil Steril. 2021. PMID: 34366109 Free PMC article.
-
Epidemiologic contributions to understanding the etiology of uterine leiomyomata.Environ Health Perspect. 2000 Oct;108 Suppl 5:821-7. doi: 10.1289/ehp.00108s5821. Environ Health Perspect. 2000. PMID: 11035989 Review.
-
Leiomyomata: heritability and cytogenetic studies.Hum Reprod Update. 2001 Jan-Feb;7(1):8-14. doi: 10.1093/humupd/7.1.8. Hum Reprod Update. 2001. PMID: 11212080 Review.
Cited by
-
Racial disparity in uterine leiomyoma: new insights of genetic and environmental burden in myometrial cells.Mol Hum Reprod. 2024 Feb 29;30(3):gaae004. doi: 10.1093/molehr/gaae004. Mol Hum Reprod. 2024. PMID: 38290796 Free PMC article. Review.
-
A Prospective Ultrasound Study of Whole Blood Metals and Incidence of Uterine Leiomyomata.Environ Health Perspect. 2025 Apr;133(3-4):47012. doi: 10.1289/EHP15218. Epub 2025 Apr 25. Environ Health Perspect. 2025. PMID: 40063901 Free PMC article.
-
Increased risk of atrial fibrillation in uterine fibroid patients: a nationwide population-based study.Sci Rep. 2025 Jul 31;15(1):27927. doi: 10.1038/s41598-025-12954-z. Sci Rep. 2025. PMID: 40744992 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
