

Hematopathology of Severe Acute Respiratory Syndrome Coronavirus 2 Infection and Coronavirus Disease-19
- PMID: 37149356
- PMCID: PMC9892324
- DOI: 10.1016/j.path.2023.01.007
Hematopathology of Severe Acute Respiratory Syndrome Coronavirus 2 Infection and Coronavirus Disease-19
Abstract
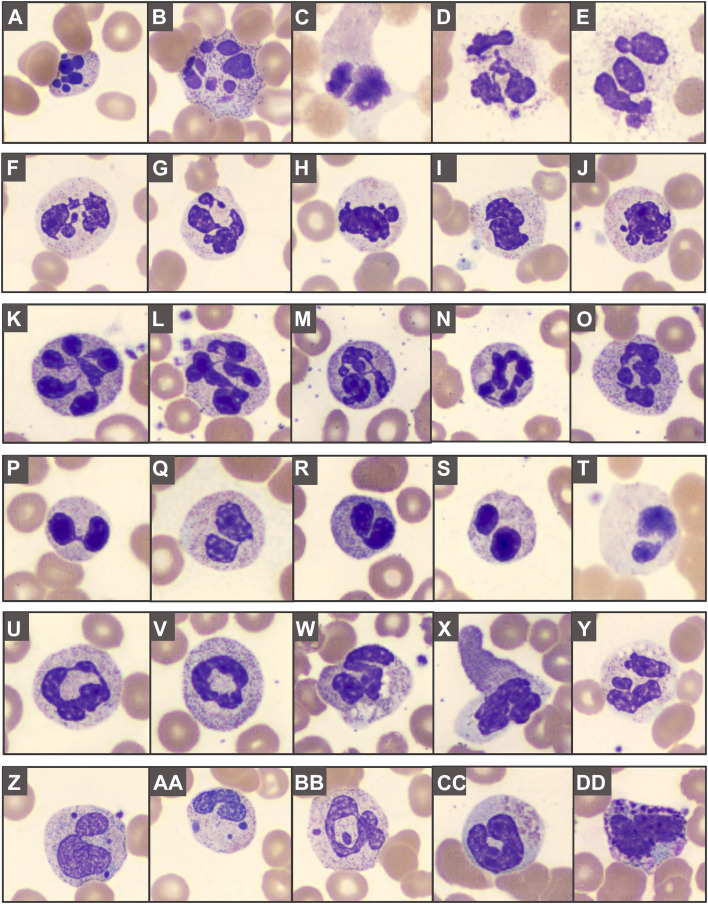
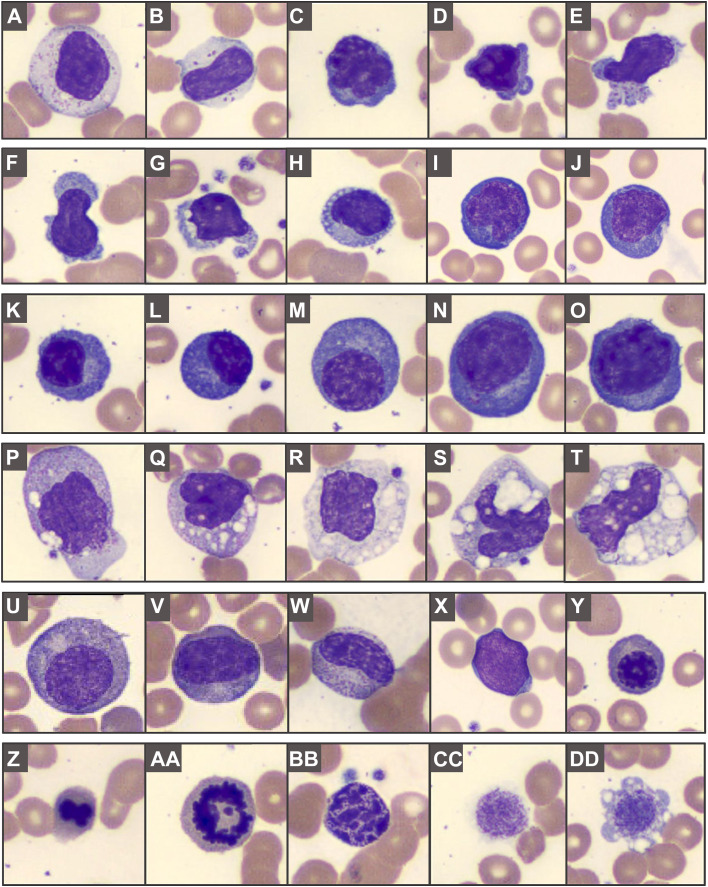
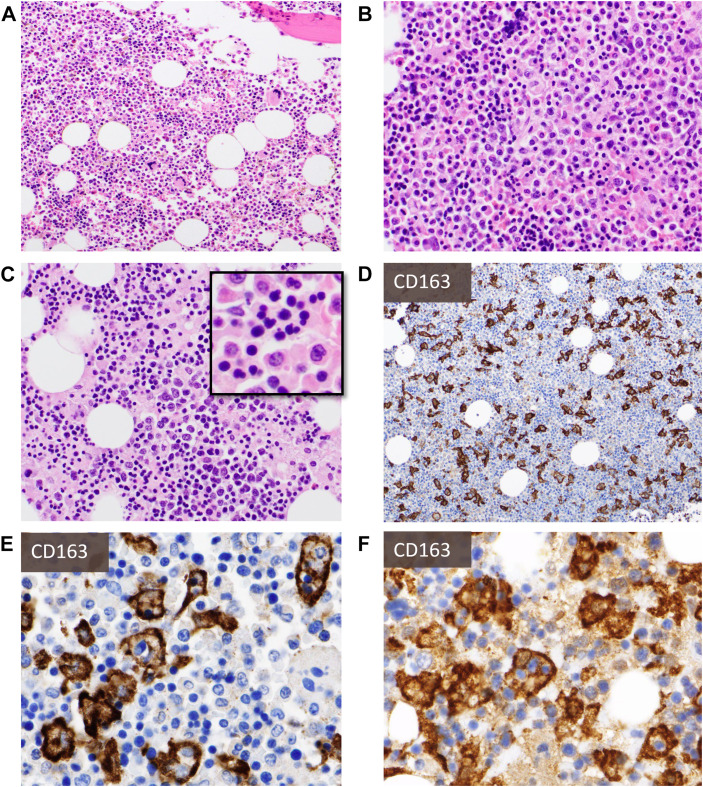
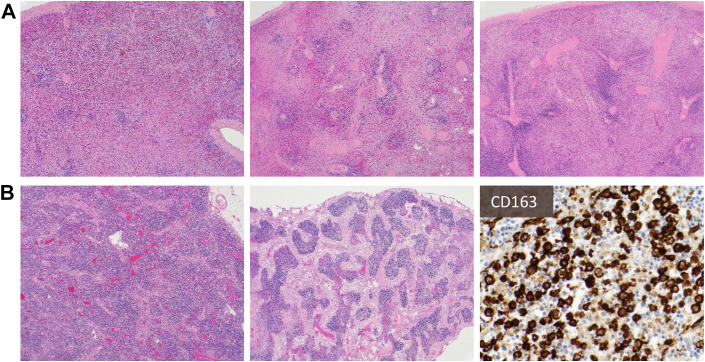
Coronavirus disease 2019 is caused by severe acute respiratory syndrome coronavirus 2 and is associated with pronounced hematopathologic findings. Peripheral blood features are heterogeneous and very often include neutrophilia, lymphopenia, myeloid left shift, abnormally segmented neutrophils, atypical lymphocytes/plasmacytoid lymphocytes, and atypical monocytes. Bone marrow biopsies and aspirates are often notable for histiocytosis and hemophagocytosis, whereas secondary lymphoid organs may exhibit lymphocyte depletion, pronounced plasmacytoid infiltrates, and hemophagocytosis. These changes are reflective of profound innate and adaptive immune dysregulation, and ongoing research efforts continue to identify clinically applicable biomarkers of disease severity and outcome.
Keywords: Atypical lymphocytes; COVID-19; Dysgranulopoiesis; Hemophagocytic lymphohistiocytosis; Lymphadenopathy; Lymphopenia; Neutrophilia; SARS-CoV-2.
Copyright © 2023 Elsevier Inc. All rights reserved.
Figures
References
-
- Hooper J.E., Padera R.F., Dolhnikoff M., et al. A Postmortem Portrait of the Coronavirus Disease 2019 (COVID-19) Pandemic: A Large Multi-institutional Autopsy Survey Study. Arch Pathol Lab Med. 2021;145(5):529–535. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
