

Differential immunophenotype of circulating monocytes from pregnant women in response to viral ligands
- PMID: 37149573
- PMCID: PMC10163583
- DOI: 10.1186/s12884-023-05562-0
Differential immunophenotype of circulating monocytes from pregnant women in response to viral ligands
Abstract
Background: Viral infections during pregnancy can have deleterious effects on mothers and their offspring. Monocytes participate in the maternal host defense against invading viruses; however, whether pregnancy alters monocyte responses is still under investigation. Herein, we undertook a comprehensive in vitro study of peripheral monocytes to characterize the differences in phenotype and interferon release driven by viral ligands between pregnant and non-pregnant women.
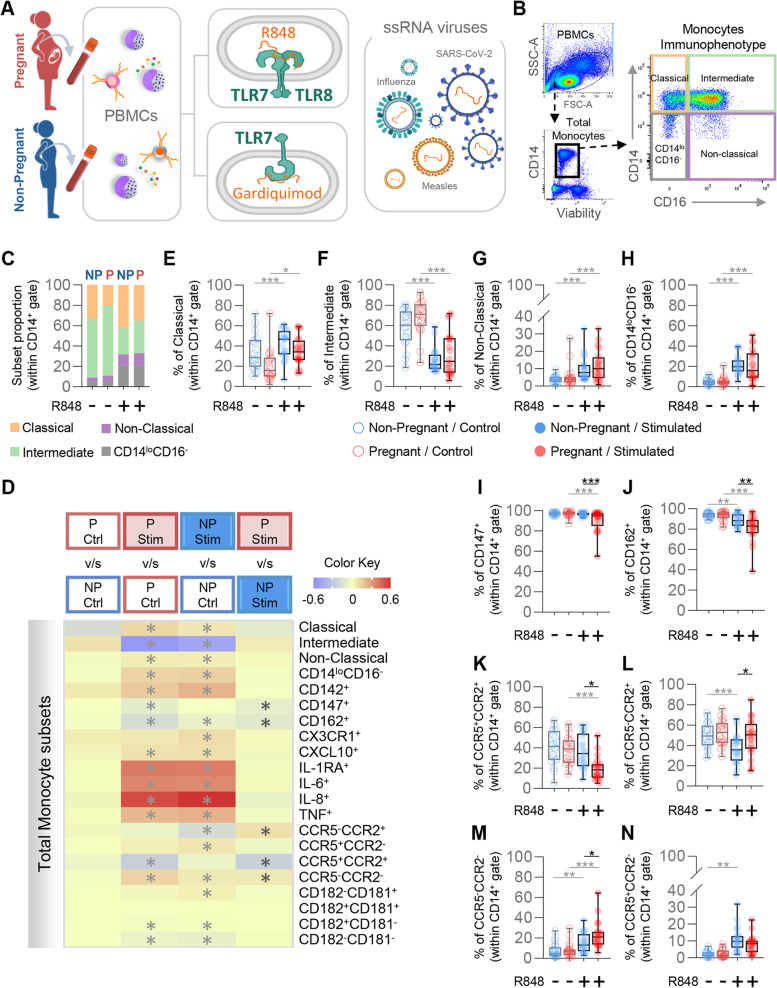
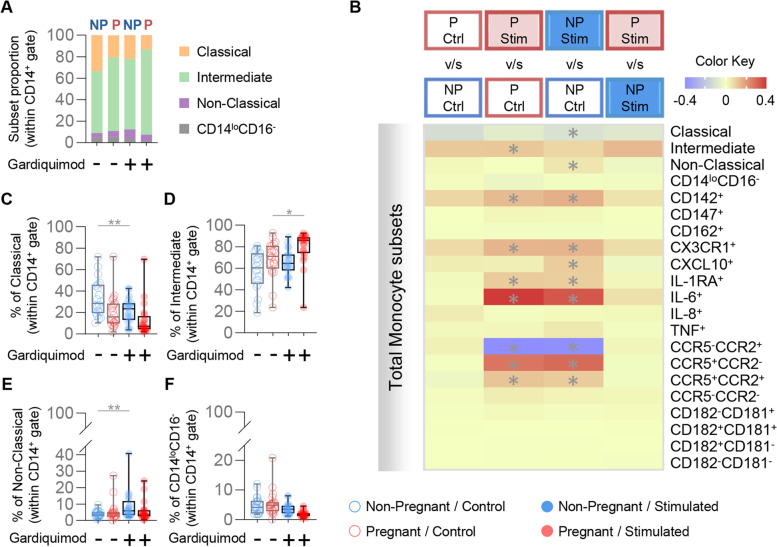
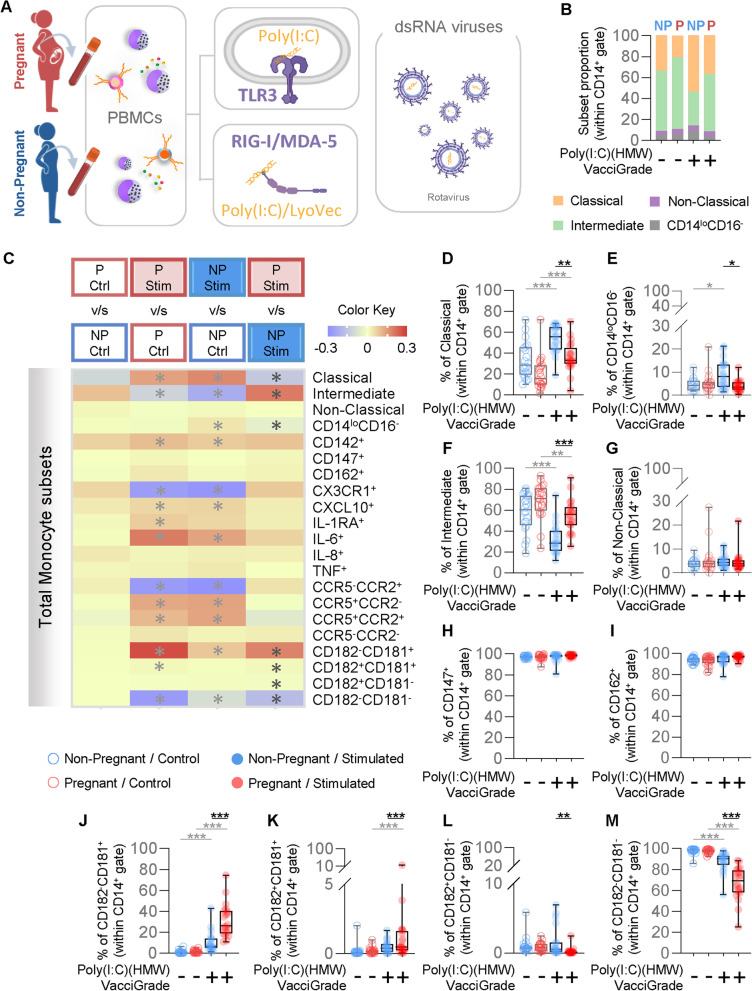
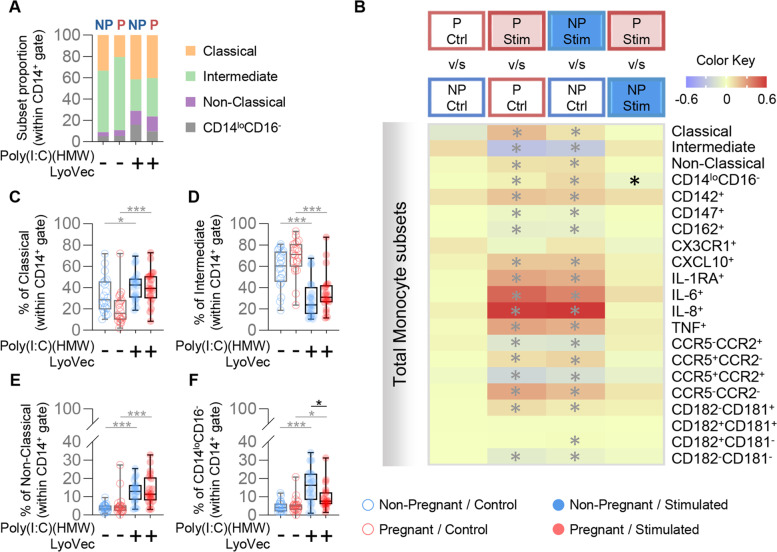
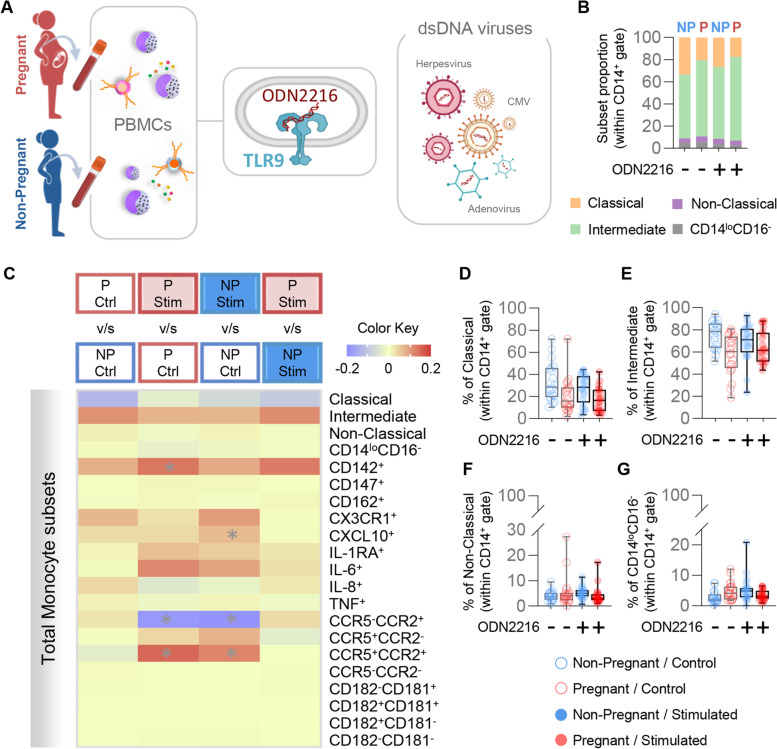
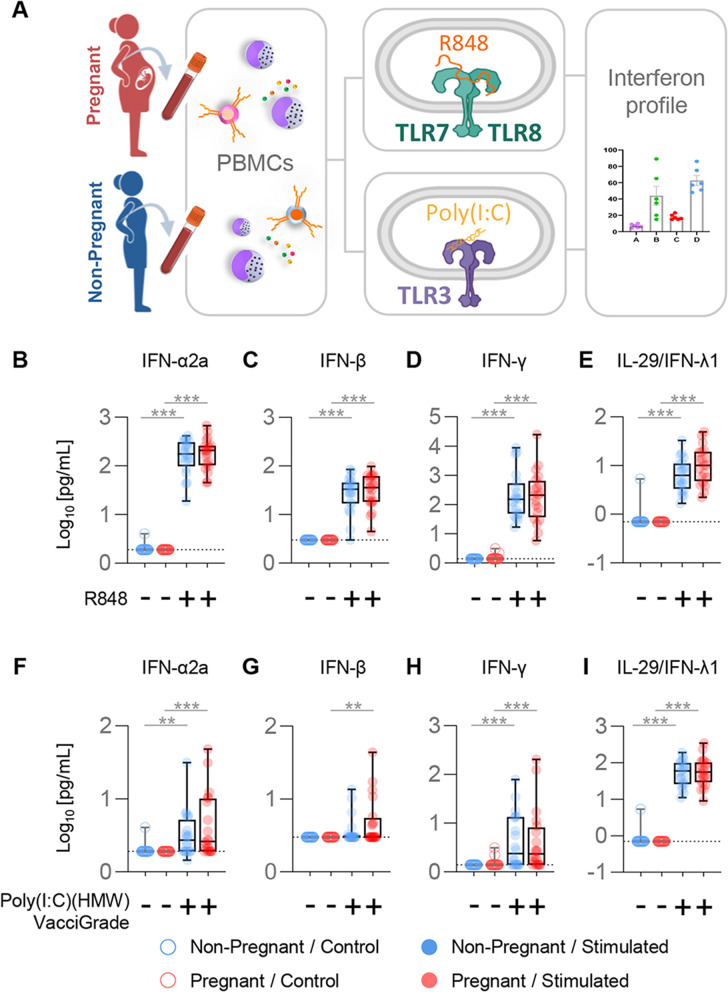
Methods: Peripheral blood was collected from third-trimester pregnant (n = 20) or non-pregnant (n = 20, controls) women. Peripheral blood mononuclear cells were isolated and exposed to R848 (TLR7/TLR8 agonist), Gardiquimod (TLR7 agonist), Poly(I:C) (HMW) VacciGrade™ (TLR3 agonist), Poly(I:C) (HMW) LyoVec™ (RIG-I/MDA-5 agonist), or ODN2216 (TLR9 agonist) for 24 h. Cells and supernatants were collected for monocyte phenotyping and immunoassays to detect specific interferons, respectively.
Results: The proportions of classical (CD14hiCD16-), intermediate (CD14hiCD16+), non-classical (CD14loCD16+), and CD14loCD16- monocytes were differentially affected between pregnant and non-pregnant women in response to TLR3 stimulation. The proportions of pregnancy-derived monocytes expressing adhesion molecules (Basigin and PSGL-1) or the chemokine receptors CCR5 and CCR2 were diminished in response to TLR7/TLR8 stimulation, while the proportions of CCR5- monocytes were increased. Such differences were found to be primarily driven by TLR8 signaling, rather than TLR7. Moreover, the proportions of monocytes expressing the chemokine receptor CXCR1 were increased during pregnancy in response to poly(I:C) stimulation through TLR3, but not RIG-I/MDA-5. By contrast, pregnancy-specific changes in the monocyte response to TLR9 stimulation were not observed. Notably, the soluble interferon response to viral stimulation by mononuclear cells was not diminished in pregnancy.
Conclusions: Our data provide insight into the differential responsiveness of pregnancy-derived monocytes to ssRNA and dsRNA, mainly driven by TLR8 and membrane-bound TLR3, which may help to explain the increased susceptibility of pregnant women to adverse outcomes resulting from viral infection as observed during recent and historic pandemics.
Keywords: Human; Infection; Innate immunity; Pregnancy; Virus.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Gibson CS, Goldwater PN, MacLennan AH, Haan EA, Priest K, Dekker GA, et al. Fetal exposure to herpesviruses may be associated with pregnancy-induced hypertensive disorders and preterm birth in a Caucasian population. BJOG. 2008;115(4):492–500. doi: 10.1111/j.1471-0528.2007.01653.x. - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
