

The status of low anterior resection syndrome: data from a single-center in China
- PMID: 37149588
- PMCID: PMC10164312
- DOI: 10.1186/s12893-023-02008-4
The status of low anterior resection syndrome: data from a single-center in China
Abstract
Aim: The incidence and risk factors of low anterior resection syndrome (LARS) largely variate in different studies. In addition, there is lack of study on how patients evaluate the therapeutic effect of LARS. This single-center retrospective study aims to investigate the status of LARS in Chinese patients undergoing laparoscopic low anterior resection (LAR).
Methods: Consequent patients undergoing laparoscopic LAR and free from disease recurrence from January 2015 to May 2021 were issued with both LARS questionnaire and satisfaction survey. Related data were collected and analyzed.
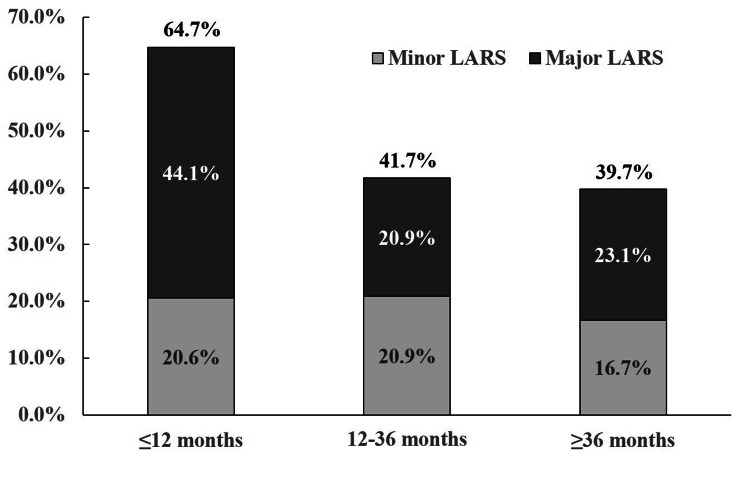
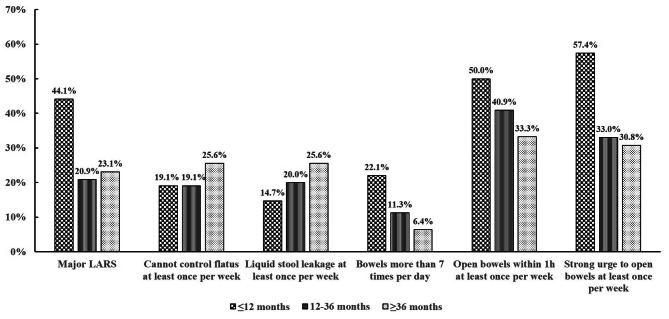
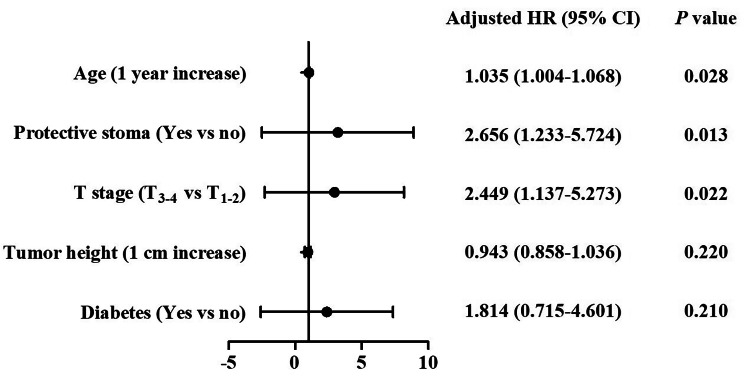
Results: Both LARS questionnaires and self-made satisfaction survey were received from 261 eligible patients. The overall incidence of LARS was 47.1% (minor in 19.5%, major in 27.6%), decreased with the passage of postoperative time (64.7% within 12 months, and 41.7% within 12-36 months), and became stable 36 months later (39.7%). The most common symptoms were defecation clustering (n = 107/261, 41.0%) and defecation urgency (n = 101/261, 38.7%). According to the multivariable regression analysis, risk factors of major LARS were: 1 year increase in age (OR 1.035, 95% CI 1.004-1.068), protective stoma (OR 2.656, 95% CI 1.233-5.724) and T3 - 4 stage (OR 2.449, 95% CI 1.137-5.273). Most patients complained defecation disorder (87.3%) to doctors and 84.5% got suggestions or treatments for it. However, only 36.8% patients thought the treatments worked for them.
Conclusions: LARS frequently occurs after laparoscopic LAR, while the therapeutic effect is not satisfying. Elder, advanced T-stage and protective stoma were risk factors for postoperative major LARS.
Keywords: Bowel dysfunction; Low anterior resection syndrome; Quality of life; Rectal neoplasms; Satisfaction survey.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
