

Fluid Optimisation in Emergency Laparotomy (FLO-ELA) Trial: study protocol for a multi-centre randomised trial of cardiac output-guided fluid therapy compared to usual care in patients undergoing major emergency gastrointestinal surgery
- PMID: 37149623
- PMCID: PMC10163929
- DOI: 10.1186/s13063-023-07275-3
Fluid Optimisation in Emergency Laparotomy (FLO-ELA) Trial: study protocol for a multi-centre randomised trial of cardiac output-guided fluid therapy compared to usual care in patients undergoing major emergency gastrointestinal surgery
Abstract
Introduction: Postoperative morbidity and mortality in patients undergoing major emergency gastrointestinal surgery are a major burden on healthcare systems. Optimal management of perioperative intravenous fluids may reduce mortality rates and improve outcomes from surgery. Previous small trials of cardiac-output guided haemodynamic therapy algorithms in patients undergoing gastrointestinal surgery have suggested this intervention results in reduced complications and a modest reduction in mortality. However, this existing evidence is based mainly on elective (planned) surgery, with little evaluation in the emergency setting. There are fundamental clinical and pathophysiological differences between the planned and emergency surgical setting which may influence the effects of this intervention. A large definitive trial in emergency surgery is needed to confirm or refute the potential benefits observed in elective surgery and to inform widespread clinical practice.
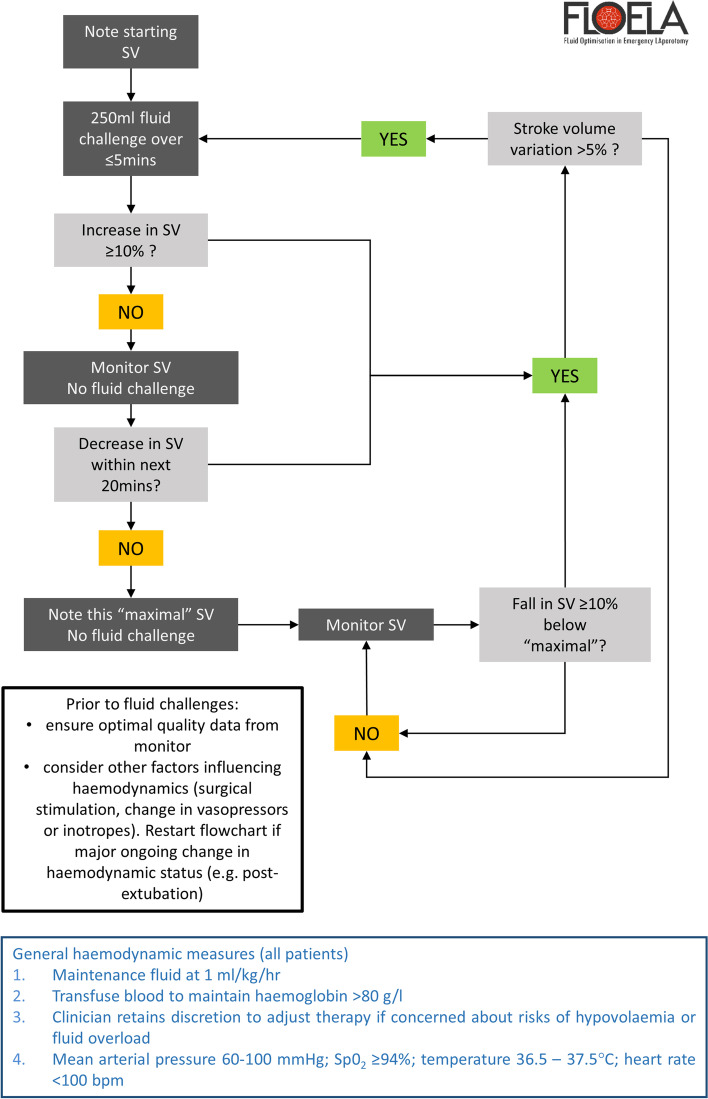
Methods: The FLO-ELA trial is a multi-centre, parallel-group, open, randomised controlled trial. 3138 patients aged 50 and over undergoing major emergency gastrointestinal surgery will be randomly allocated in a 1:1 ratio using minimisation to minimally invasive cardiac output monitoring to guide protocolised administration of intra-venous fluid, or usual care without cardiac output monitoring. The trial intervention will be carried out during surgery and for up to 6 h postoperatively. The trial is funded through an efficient design call by the National Institute for Health and Care Research Health Technology Assessment (NIHR HTA) programme and uses existing routinely collected datasets for the majority of data collection. The primary outcome is the number of days alive and out of hospital within 90 days of randomisation. Participants and those delivering the intervention will not be blinded to treatment allocation. Participant recruitment started in September 2017 with a 1-year internal pilot phase and is ongoing at the time of publication.
Discussion: This will be the largest contemporary randomised trial examining the effectiveness of perioperative cardiac output-guided haemodynamic therapy in patients undergoing major emergency gastrointestinal surgery. The multi-centre design and broad inclusion criteria support the external validity of the trial. Although the clinical teams delivering the trial interventions will not be blinded, significant trial outcome measures are objective and not subject to detection bias.
Trial registration: ISRCTN 14729158. Registered on 02 May 2017.
Keywords: Emergency surgical procedures/adverse effects; Hemodynamics/physiology; Intraoperative/methods; Postoperative complications/prevention and control; Prospective studies.
© 2023. The Author(s).
Conflict of interest statement
MRE has received an honorarium for lecturing for Edwards Lifesciences and is Deputy Chief Investigator of the OPTIMISE II trial of cardiac output-guided haemodynamic therapy in patients undergoing elective gastrointestinal surgery (funded by NIHR and Edwards Lifesciences although does not receive any financial support in this role). MPWG reports serving as Medical Advisory Board, Sphere Medical Ltd; Medical Advisory Board and consultancy work (outside the submitted work) for Edwards Lifesciences; Director, EBPOM Social Enterprise; Director, Oxygen Control Systems Ltd; Director, EBPOM USA; Director, NIHR Southampton Biomedical Research Centre; and Joint Editor-in-Chief, Perioperative Medicine. MGM reports personal fees from Deltex Medical, personal fees from Edwards Lifesciences, personal fees from Baxter, and grants from Smiths Medical, outside the submitted work. In addition, MGM has a patent “QUENCH” a patient hydration device (issued). RMP has received research grants and/or honoraria from Edwards Lifesciences, Intersurgical and GlaxoSmithKline. DGM reports serving as an NIHR Senior Investigator.
GF, NW, BM, MT, RP, KY, AT, BCK, MH, DM, and IA declare that they have no competing interests.
Figures
References
-
- NELA project team. First patient report of the national emergency laparotomy audit. London: Royal College of Anaesthetists; 2015. Available from: http://nela.org.uk/reports.
-
- NELA project team . The second patient report of the national emergency laparotomy audit. 2016.
-
- Oliver CM, Bassett MG, Poulton TE, Anderson ID, Murray DM, Grocott MP, et al. Organisational factors and mortality after an emergency laparotomy: multilevel analysis of 39 903 National Emergency Laparotomy Audit patients. Br J Anaesth. 2018;121(6):1346–1356. doi: 10.1016/j.bja.2018.07.040. - DOI - PubMed
-
- Peden CJ, Stephens T, Martin G, Kahan BC, Thomson A, Rivett K, et al. Effectiveness of a national quality improvement programme to improve survival after emergency abdominal surgery (EPOCH): a stepped-wedge cluster-randomised trial. Lancet Lond Engl. 2019;393(10187):2213–21. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
