

Post COVID-19 condition after delta infection and omicron reinfection in children and adolescents
- PMID: 37149931
- PMCID: PMC10166589
- DOI: 10.1016/j.ebiom.2023.104599
Post COVID-19 condition after delta infection and omicron reinfection in children and adolescents
Abstract
Background: The burden of COVID-19 in children and adolescents has increased during the delta and omicron waves, necessitating studies of long-term symptoms such as fatigue, dyspnoea and cognitive problems. Furthermore, immune responses in relation to persisting symptoms in younger people have not been well characterised. In this cohort study, we investigated the role of antibodies, vaccination and omicron reinfection upon persisting and long-term symptoms up to 8 months post-delta infection.
Methods: SARS-CoV-2 RT-PCR positive participants (n = 276, aged 10-20 years) were prospectively recruited in August 2021. We recorded the major symptoms of post COVID-19 condition and collected serum samples 3- and 8-months post delta infection. Binding antibodies were measured by spike IgG ELISA, and surrogate neutralising antibodies against Wuhan and delta variants by the hemagglutination test (HAT).
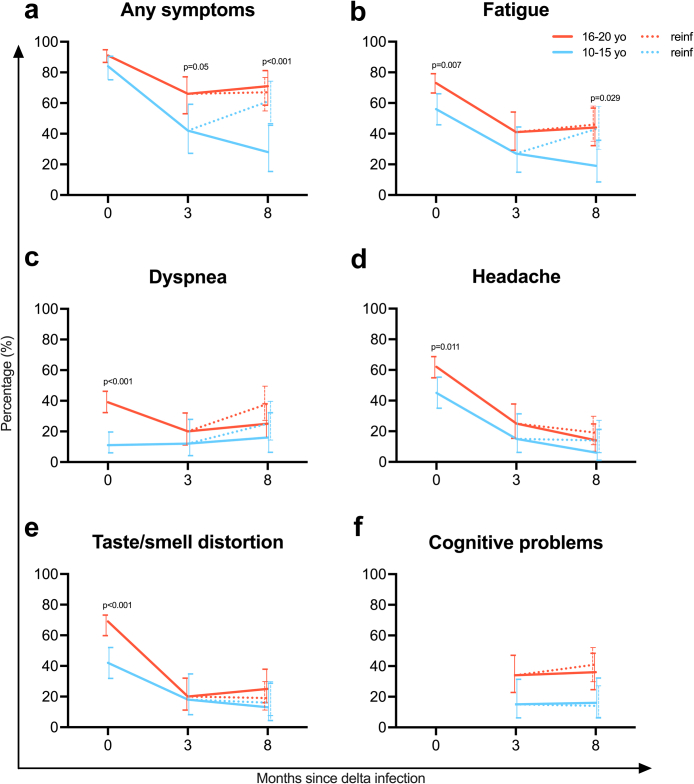
Findings: After delta infection, persisting symptoms at 3 months were significantly associated with higher delta antibody titres (OR 2.97, 95% CI 1.57-6.04, p = 0.001). Asymptomatic acute infection compared to symptomatic infection lowered the risk of persisting (OR 0.13, 95% CI 0.02-0.55, p = 0.013) and long-term (OR 0.28 95% CI 0.11-0.66, p = 0.005) symptoms at 3 and 8 months, respectively. Adolescents (16-20 years) were more likely to have long-term symptoms compared to children (10-15 years) (OR 2.44, 95% CI 1.37-4.41, p = 0.003).
Interpretation: This clinical and serological study compares long-term symptoms after delta infection between children and adolescents. The association between high antibody titres and persisting symptoms suggest the involvement of an immune mechanism. Similarly to adults, the dominant long-term symptoms in children are fatigue, dyspnoea and cognitive problems.
Funding: This work was funded by the Ministry of Health and Care Services, Norway, the University of Bergen, Norway and Helse Vest, Norway (F-12621).
Keywords: Antibody; Children and adolescents; Delta variant; Omicron variant; Post COVID-19 condition; SARS-CoV-2 infection.
Copyright © 2023 The Author(s). Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of interests All authors declare no conflict of interest.
Figures



References
-
- World Health Organization A clinical case definition of post COVID-19 condition by a Delphi consensus, 6 October 2021 who.int 2021 [updated 6 October 2021. https://www.who.int/publications/i/item/WHO-2019-nCoV-Post_COVID-19_cond... Available from:
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
