

Necrotizing fasciitis of the chest wall caused by empyema necessitans following tuberculosis: Case report and literature review
- PMID: 37150161
- PMCID: PMC10195979
- DOI: 10.1016/j.ijscr.2023.108300
Necrotizing fasciitis of the chest wall caused by empyema necessitans following tuberculosis: Case report and literature review
Abstract
Introduction and importance: Empyema is a serious complication characterized by pus and bacteria in the pleural space which may progress to necrosis, cavitation, or fistulas in the thoracic cavity. Infection and trauma are the commonest causes in the developed countries while tuberculosis is the commonest cause of empyema in developing countries. Empyema necessitans is a rare complication of pleural space infections.
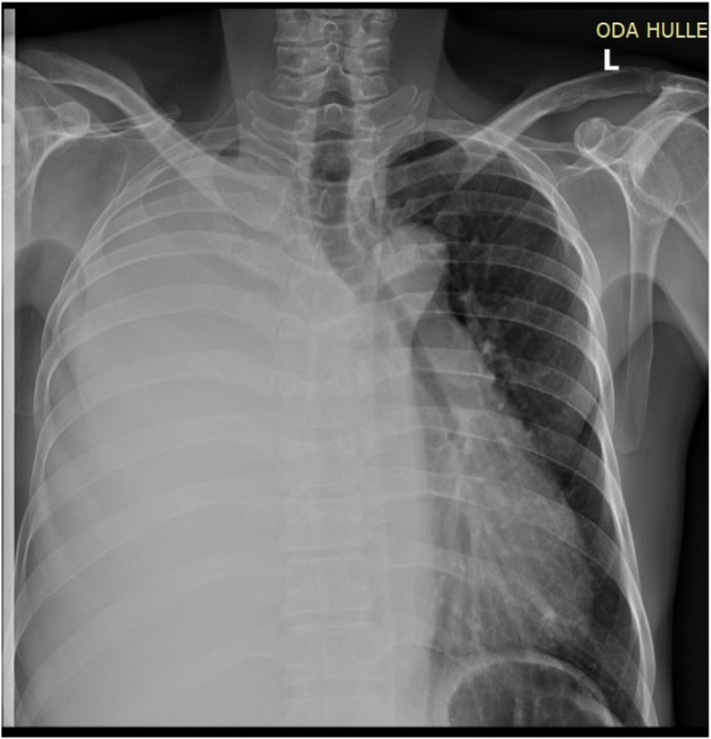
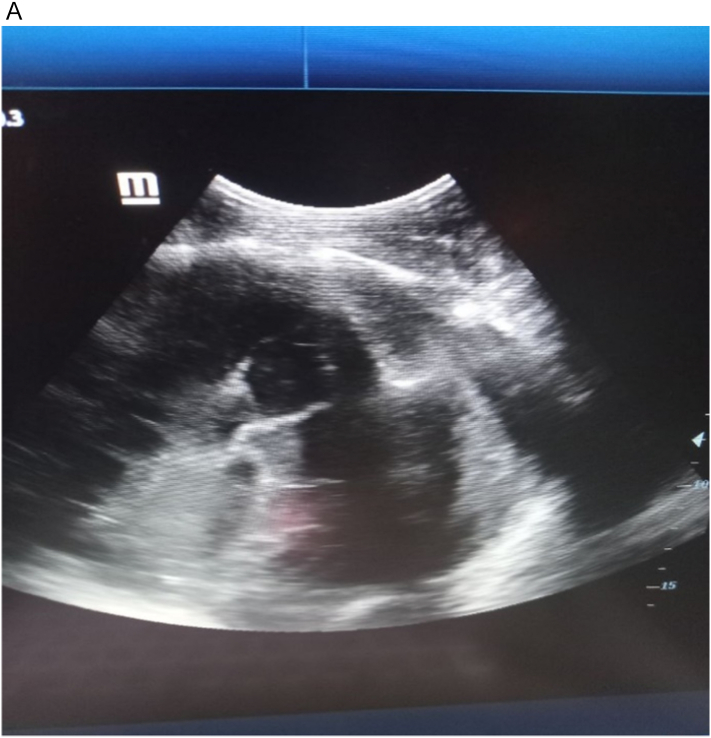
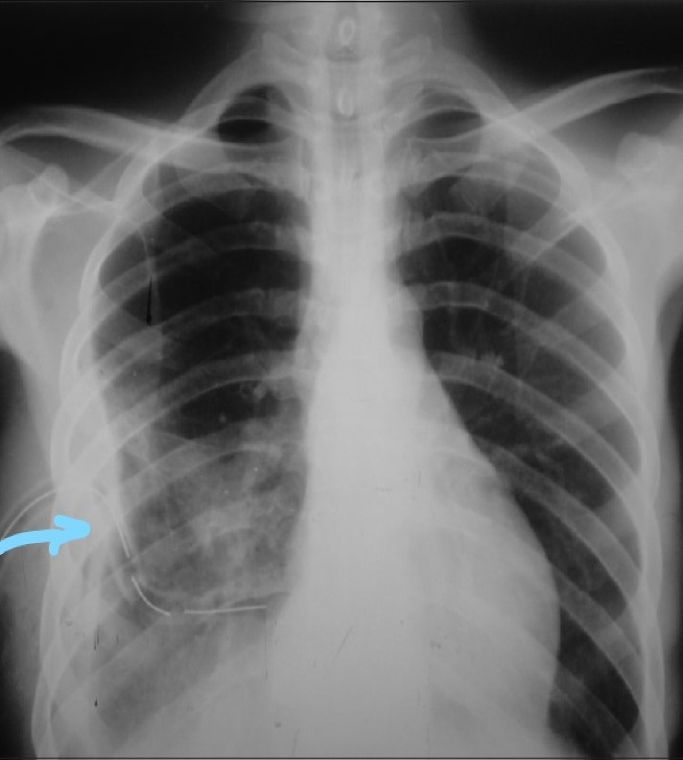
Case presentation: A 50 years old male patient presented to our hospital with right side chest pain and shortness of breath of 3-week duration. He had completed treatment of pulmonary tuberculosis 6 months ago. The patient was apparently healthy for the last six months after the treatment. The patient was acutely sick looking and has tachycardia with pulse rate of 115, respiratory rate was 36 and arterial oxygen saturation of 80 % with atmospheric air but becomes 96 % with facemask humidified oxygen. Tube thoracostomy and chest wall debridement was done for empyema necessitans with chest wall necrotizing fasciitis.
Clinical discussion: Empyematous collection with time may lead to a more complicated scenario called empyema necessitans. Empyema necessitans is the dissection of puss thru the pleural space and collection in the torso/ free rupture with or without collection of air. The most common cause of empyema globally is untreated parapneumonic effusion. Tuberculosis constitutes for most of the cases of empyema necessitans in third world countries. Debridement and wound care are monumental for the management of necrotizing fasciitis in addition to broad spectrum antibiotics.
Conclusion: Timely treatment/drug adherence to pneumonia and tuberculosis decreases the rate of having empyema and subsequent complication. Chest wall necrotizing fasciitis is extremely rare and judicious management with debridement and wound care is appropriate whenever it happens. Broad spectrum antibiotics with drainage are the norm of management of empyema/empyema necessitans.
Keywords: Case report; Empyema; Empyema necessitans; Necrotizing fasciitis; Tuberculosis.
Copyright © 2023 The Author(s). Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Competing interest The author declares that there are no competing interests.
Figures






Similar articles
-
Empyema Necessitans: A Rare Complication of Chest Drains.Cureus. 2024 Sep 22;16(9):e69931. doi: 10.7759/cureus.69931. eCollection 2024 Sep. Cureus. 2024. PMID: 39439608 Free PMC article.
-
Persistent pleural tuberculosis presenting as chest wall swellings in an immunocompetent patient: A rare case report in a low resource setting.Int J Surg Case Rep. 2025 Jan;126:110674. doi: 10.1016/j.ijscr.2024.110674. Epub 2024 Nov 26. Int J Surg Case Rep. 2025. PMID: 39608329 Free PMC article.
-
Empyema Necessitans: A Case Report.IDCases. 2024 Apr 2;36:e01939. doi: 10.1016/j.idcr.2024.e01939. eCollection 2024. IDCases. 2024. PMID: 38601432 Free PMC article.
-
Empyema necessitans caused by methicillin-resistant Staphylococcus aureus: a case report and literature review.BMC Infect Dis. 2024 Feb 1;24(1):157. doi: 10.1186/s12879-024-09062-0. BMC Infect Dis. 2024. PMID: 38302885 Free PMC article. Review.
-
Unusual presentation of empyema necessitans: case report and review of the literature.Gen Thorac Cardiovasc Surg. 2021 Jun;69(6):1026-1030. doi: 10.1007/s11748-021-01601-9. Epub 2021 Feb 9. Gen Thorac Cardiovasc Surg. 2021. PMID: 33559044 Review.
Cited by
-
Tuberculous Necrotizing Fasciitis in a Patient with Rheumatoid Arthritis on Anti-TNF Treatment: A Case Report.Eur J Rheumatol. 2025 Feb 17;12(1):1-4. doi: 10.5152/eurjrheum.2025.23035. Eur J Rheumatol. 2025. PMID: 40177742 Free PMC article.
-
Empyema necessitans in a pediatric patient: A case study.Int J Surg Case Rep. 2023 Nov;112:108932. doi: 10.1016/j.ijscr.2023.108932. Epub 2023 Oct 14. Int J Surg Case Rep. 2023. PMID: 37856970 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources
