

Tirzepatide and prevention of chronic kidney disease
- PMID: 37151412
- PMCID: PMC10157759
- DOI: 10.1093/ckj/sfac274
Tirzepatide and prevention of chronic kidney disease
Abstract
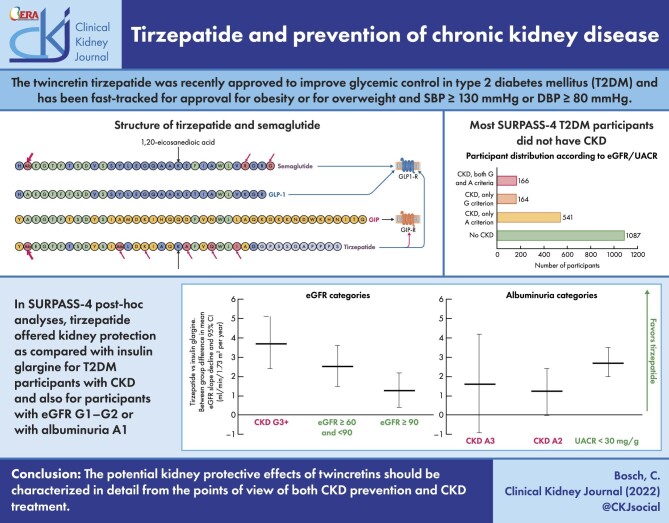
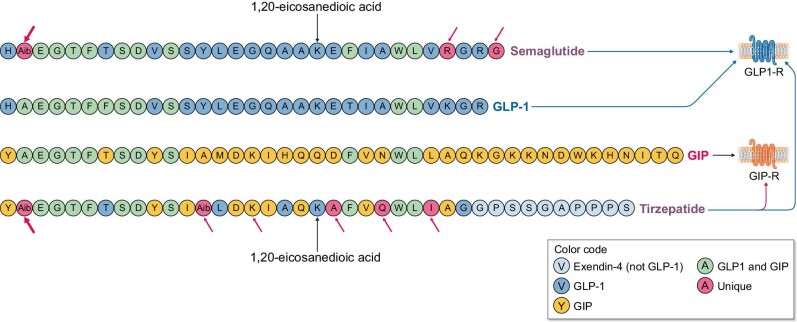
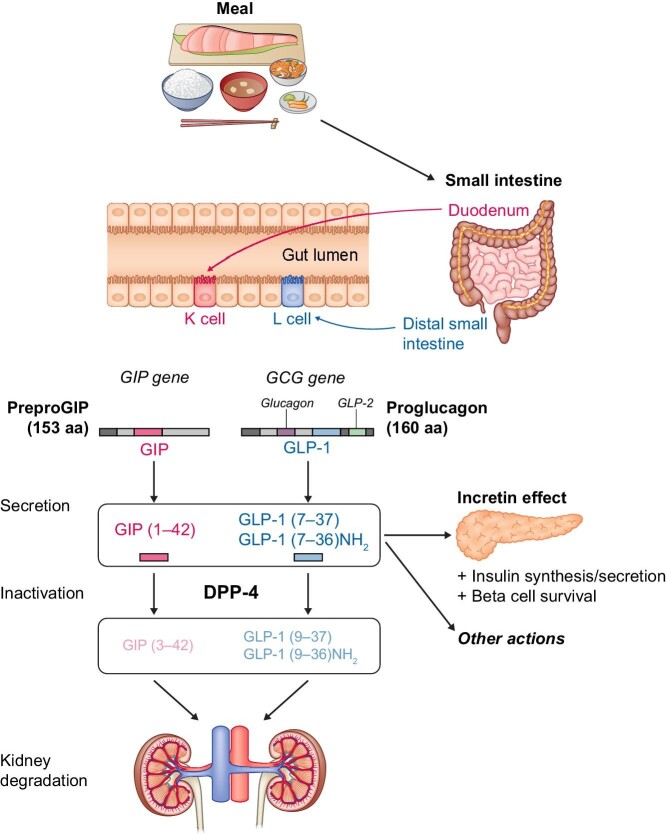
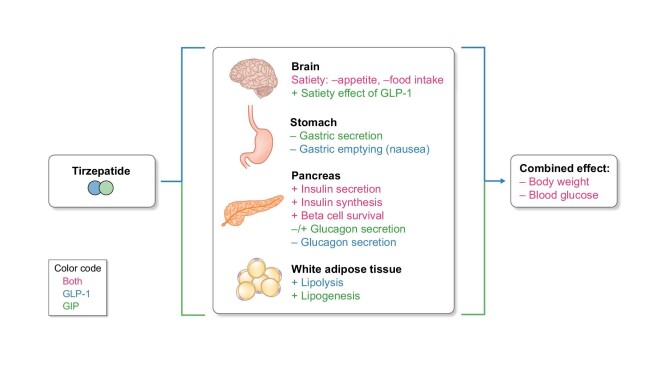
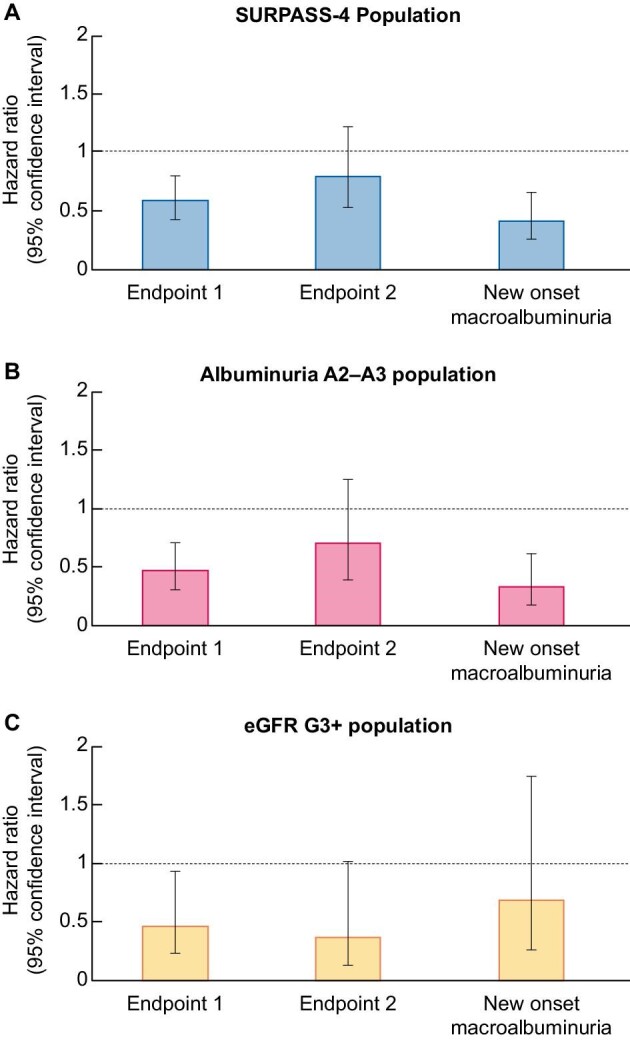
Tirzepatide is a twincretin recently approved to improve glycemic control in type 2 diabetes mellitus (T2DM). More specifically, tirzepatide is an agonist of both the glucose-dependent insulinotropic polypeptide (GIP) and the glucagon-like peptide-1 (GLP1) receptors. In recent clinical trials in persons with obesity or overweight with associated conditions, tirzepatide decreased body weight and other cardiorenal risk factors (blood pressure, low-density lipoprotein cholesterol, glycated hemoglobin and albuminuria). Moreover, in a post hoc analysis of the SURPASS-4 randomized clinical trial, tirzepatide decreased albuminuria and total estimated glomerular filtration rate (eGFR) slopes and nearly halved the risk of a pre-specified composite kidney endpoint (eGFR decline ≥40%, renal death, kidney failure or new-onset macroalbuminuria) in participants with T2DM and high cardiovascular risk when compared with insulin glargine. Similar to other kidney-protective drugs, tirzepatide, alone or combined with sodium-glucose co-transporter 2 inhibitors, caused an early dip in eGFR. Moreover, tirzepatide also decreased eGFR slopes in participants with eGFR >60 mL/min/1.73 m2 or with normoalbuminuria. We now review the potential kidney health implications of tirzepatide, addressing its structure and function, relationship to current GLP1 receptor agonists, impact of recent results for the treatment and prevention of kidney disease, and expectations for the future.
Keywords: chronic kidney disease; diabetes mellitus; incretin; obesity; tirzepatide.
© The Author(s) 2022. Published by Oxford University Press on behalf of the ERA.
Conflict of interest statement
A.O. is the former Editor-in-Chief of CKJ and has received grants from Sanofi and consultancy or speaker fees or travel support from Advicciene, Astellas, AstraZeneca, Amicus, Amgen, Fresenius Medical Care, GSK, Bayer, Sanofi-Genzyme, Menarini, Mundipharma, Kyowa Kirin, Alexion, Freeline, Idorsia, Chiesi, Otsuka, Novo-Nordisk, Sysmex and Vifor Fresenius Medical Care Renal Pharma and is Director of the Catedra Mundipharma-UAM of diabetic kidney disease and the Catedra AstraZeneca-UAM of chronic kidney disease and electrolytes. B.F.-F. has received grants from Esteve and consultancy or speaker fees or travel support from AstraZeneca, Bayer, Menarini, Novo-Nordisk Boehringer Ingelheim and Mundipharma. B.F.-F. is Editor for Nefroplus. S.C. has received honoraria for consultancy from Otsuka. M.J.S. is the Editor-in-Chief of CKJ and reports personal fees from NovoNordisk, Jansen, Mundipharma, AstraZeneca, Esteve, Fresenius, Ingelheim Lilly, Vifor, ICU, Pfizer, Bayer, Travere Therapeutics and GE Healthcare, and grants and personal fees from Boehringer Ingelheim, outside the current study.
Figures

References
-
- MounjaroTM (tirzepatide) prescribing information. https://www.accessdata.fda.gov/drugsatfda_docs/label/2022/215866s000lbl.pdf (9 July 2022, date last accessed).
-
- Jastreboff AM, Aronne LJ, Ahmad NN et al. Tirzepatide once weekly for the treatment of obesity. N Engl J Med 2022;387:205–16. - PubMed
-
- Heerspink HJL, Sattar N, Pavo I et al. Effects of tirzepatide versus insulin glargine on kidney outcomes in type 2 diabetes in the SURPASS-4 trial: post-hoc analysis of an open-label, randomised, phase 3 trial. Lancet Diabetes Endocrinol 2022;10:774–85. - PubMed
-
- Wegovy. Summary of products characteristics, https://www.ema.europa.eu/en/documents/product-information/wegovy-epar-p... (9 July 2022, date last accessed).
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
