

Cost modelling incorporating procalcitonin for the risk stratification of febrile infants ≤60 days old
- PMID: 37151930
- PMCID: PMC10156926
- DOI: 10.1093/pch/pxac083
Cost modelling incorporating procalcitonin for the risk stratification of febrile infants ≤60 days old
Abstract
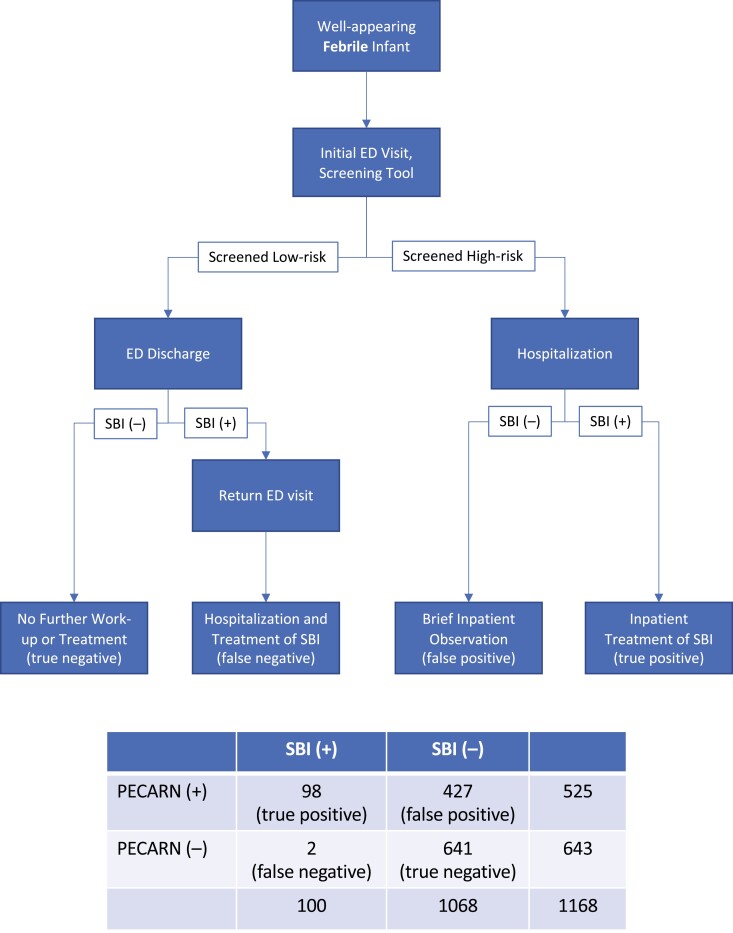
Objectives: Procalcitonin testing is recommended to discriminate febrile young infants at risk of serious bacterial infections (SBI). However, this test is not available in many clinical settings, limited largely by cost. This study sought to evaluate contemporary real-world costs associated with the usual care of febrile young infants, and estimate impact on clinical trajectory and costs when incorporating procalcitonin testing.
Methods: We assessed hospital-level door-to-discharge costs of all well-appearing febrile infants aged ≤60 days, evaluated at a tertiary paediatric hospital between April/2016 and March/2019. Emergency Department and inpatient expense data for usual care were obtained from the institutional general ledger, validated by the provincial Ministry of Health. These costs were then incorporated into a probabilistic model of risk stratification for an equivalent simulated cohort, with the addition of procalcitonin.
Results: During the 3-year study period, 1168 index visits were included for analysis. Real-world median costs-per-infant were the following: $3266 (IQR $2468 to $4317, n=93) for hospitalized infants with SBIs; $2476 (IQR $1974 to $3236, n=530) for hospitalized infants without SBIs; $323 (IQR $286 to $393, n=538) for discharged infants without SBIs; and, $3879 (IQR $3263 to $5297, n=7) for discharged infants subsequently hospitalized for missed SBIs. Overall median cost-per-infant of usual care was $1555 (IQR $1244 to $2025), compared to a modelled cost of $1389 (IQR $1118 to $1797) with the addition of procalcitonin (10.7% overall cost savings; $1,816,733 versus $1,622,483). Under pessimistic and optimistic model assumptions, savings were 5.9% and 14.9%, respectively.
Conclusions: Usual care of febrile young infants is variable and resource intensive. Increased access to procalcitonin testing could improve risk stratification at lower overall costs.
Keywords: Cost analysis; Procalcitonin; Sepsis; Serious bacterial infection.
© The Author(s) 2022. Published by Oxford University Press on behalf of the Canadian Paediatric Society. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Conflict of interest statement
All authors: No reported conflicts of interest. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures
Similar articles
-
A Clinical Prediction Rule to Identify Febrile Infants 60 Days and Younger at Low Risk for Serious Bacterial Infections.JAMA Pediatr. 2019 Apr 1;173(4):342-351. doi: 10.1001/jamapediatrics.2018.5501. JAMA Pediatr. 2019. PMID: 30776077 Free PMC article.
-
Delays in Time-To-Antibiotics for Young Febrile Infants With Serious Bacterial Infections: A Prospective Single-Center Study.Front Pediatr. 2022 Apr 29;10:873043. doi: 10.3389/fped.2022.873043. eCollection 2022. Front Pediatr. 2022. PMID: 35573970 Free PMC article.
-
Procalcitonin as a marker of serious bacterial infections in febrile children younger than 3 years old.Acad Emerg Med. 2014 Feb;21(2):171-9. doi: 10.1111/acem.12316. Acad Emerg Med. 2014. PMID: 24673673
-
Febrile infant update.Curr Opin Pediatr. 2017 Jun;29(3):280-285. doi: 10.1097/MOP.0000000000000492. Curr Opin Pediatr. 2017. PMID: 28323666 Review.
-
Diagnosis and management of febrile infants (0-3 months).Evid Rep Technol Assess (Full Rep). 2012 Mar;(205):1-297. Evid Rep Technol Assess (Full Rep). 2012. PMID: 24422856 Free PMC article. Review.
Cited by
-
Procalcitonin use in febrile children attending European emergency departments: a prospective multicenter study.BMC Pediatr. 2025 Mar 1;25(1):157. doi: 10.1186/s12887-025-05483-1. BMC Pediatr. 2025. PMID: 40025449 Free PMC article.
-
The Critical Lens: It is time to start using the right test for febrile young infants.Paediatr Child Health. 2024 Sep 30;29(7):419-421. doi: 10.1093/pch/pxae069. eCollection 2024 Nov. Paediatr Child Health. 2024. PMID: 39677385
References
-
- Greenhow TL, Hung YY, Pantell RH.. Management and outcomes of previously healthy, full-term, febrile infants ages 7 to 90 days. Pediatrics 2016;138:e20160270-e. - PubMed
-
- Aronson PL, Thurm C, Alpern ER, et al. . Variation in care of the febrile young infant <90 days in US pediatric emergency departments. Pediatrics 2014;134:667–77. - PubMed
-
- Milcent K, Faesch S, Gras-Le Guen C, et al. . Use of procalcitonin assays to predict serious bacterial infection in young febrile infants. JAMA Pediatr 2016;170:62–9. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous