

Evaluation of the safety of retroperitoneal laparoscopic partial nephrectomy by investigating the perioperative indicators
- PMID: 37152056
- PMCID: PMC10154593
- DOI: 10.3389/fonc.2023.1138210
Evaluation of the safety of retroperitoneal laparoscopic partial nephrectomy by investigating the perioperative indicators
Retraction in
-
Retraction: Evaluation of the safety of retroperitoneal laparoscopic partial nephrectomy by investigating the perioperative indicators.Front Oncol. 2024 Feb 19;14:1383340. doi: 10.3389/fonc.2024.1383340. eCollection 2024. Front Oncol. 2024. PMID: 38440232 Free PMC article.
Abstract
Background: In recent years, open nephron sparing partial nephrectomy (OPN) has been gradually applied and generally accepted. Recent statistical data show that PN not only can safely and effectively preserve the functional nephron, but also has fewer complications, low local recurrence rate and no significant difference in long-term survival rate compared with nephrectomy/radical nephrectomy, which has gradually become a routine treatment for small renal cell carcinoma. Therefore, how to maximize the protection of postoperative residual renal function (RRF) and reduce the risk of CKD while achieving the ideal local and overall tumor control effect is the key to the treatment of renal cancer, and is also the focus of attention of urologists and nephrologists.
Objective: To evaluate the safety of retroperitoneal laparoscopic partial nephrectomy (RLPN) by investigating the perioperative indicators and postoperative follow-up.
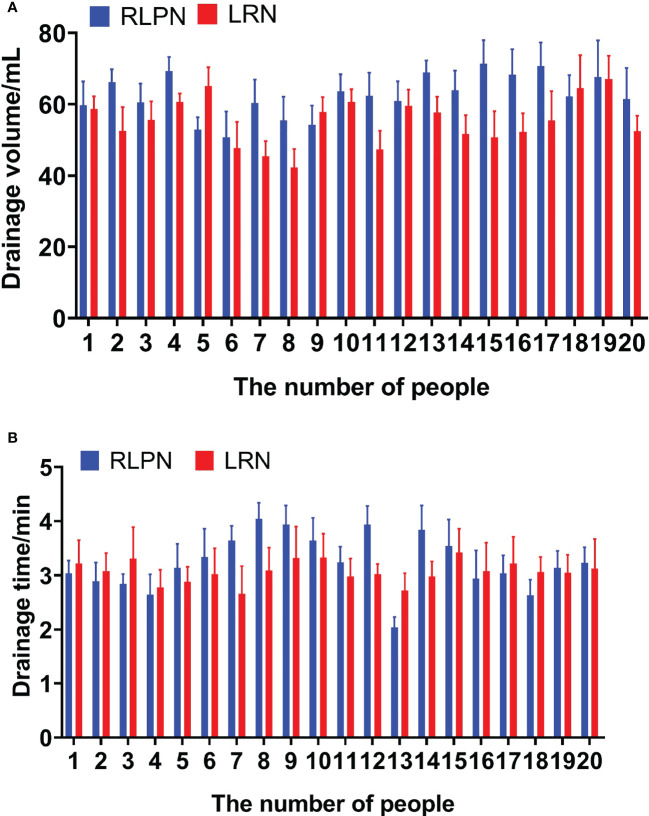
Methods: A total of 40 hospitalized patients in our hospital from December 2019 to December 2021 were selected and followed up for a long time. Patients with renal tumors less than 4cm in diameter and exogeneous or partial exogeneity were randomly divided into 2 groups. Patients in retroperitoneal laparoscopic group (n = 20) were treated with nephron sparing partial nephrectomy (0.5-1cm). Twenty patients underwent retroperitoneal laparoscopic radical nephrectomy (LRN).The time of removal of drainage tube, drainage volume, time of feeding activity and postoperative hospital stay were recorded, and the safety of the operation was evaluated.
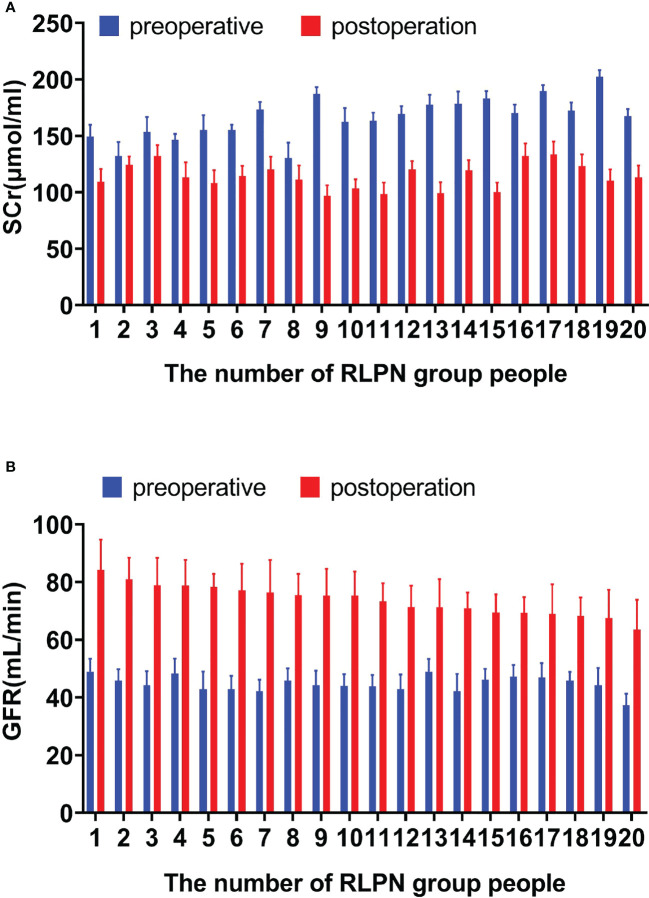
Results: nephron sparing partial nephrectomy is suitable for patients with localized renal carcinoma or benign tumor <4cm. RLPN can be applied to all indications of open nephron sparing partial nephrectomy (OPN), with good safety, and can preserve residual renal function to the greatest extent. The operative vascular occlusion time was controlled within 40 minutes, and the use of renal function protection measures during the operation was safe and controllable in reducing the prevention of warm ischemic kidney damage, with good safety. The renal tumor capsule with 0.5cm~1cm margin was complete by postoperative pathology. In the process of tumor resection and suture collection system in the RLPN group, we improved the previous operation of "resection before hemostasis" to "resection while hemostasis" and "knot-free suture" technology, which saved the operation time of intracavity suture knotting. Reduced cortical tear caused by vertical pull during knot tying. The combined effect of biological clip and hemostatic gauze can stimulate the granulation proliferation of renal cortical wound and accelerate the repair. With the combination of knot-free suture and renal segment vascular occlusion, hot ischemic kidney damage is reduced. In the RLPN group, there were no complications of urinary fistula and bleeding, and no abnormal changes in renal function during follow-up. The safety of RLPN group is worthy of affirmation.
Conclusion: The perioperative safety and short-term postoperative renal function recovery of RLPN are good, and the overall safety of this operation is worthy of affirmation.
Keywords: CT imaging; RLPN; partial resection of renal cell carcinoma; renal cell carcinoma; residual renal function.
Copyright © 2023 Zhang and Xing.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Oncologic Outcomes and Safety Assessment of Retroperitoneal Laparoscopic Partial Nephrectomy versus Open Partial Nephrectomy in Treating Patients with Localized Renal Cell Carcinoma: A Propensity Score Matching Study.Ann Ital Chir. 2024;95(5):926-933. doi: 10.62713/aic.3520. Ann Ital Chir. 2024. PMID: 39467801
-
Clinical outcomes and effect on intraoperative blood loss and postoperative pain of patients undergoing retroperitoneal laparoscopic partial nephrectomy for complex renal tumors.World J Surg Oncol. 2021 Sep 18;19(1):282. doi: 10.1186/s12957-021-02397-x. World J Surg Oncol. 2021. PMID: 34537060 Free PMC article.
-
The methods and techniques of identifying renal pedicle vessels during retroperitoneal laparoscopic radical and partial nephrectomy.World J Surg Oncol. 2019 Feb 22;17(1):38. doi: 10.1186/s12957-019-1580-1. World J Surg Oncol. 2019. PMID: 30795777 Free PMC article.
-
Laparoscopic partial nephrectomy.J Endourol. 2005 Jul-Aug;19(6):634-42. doi: 10.1089/end.2005.19.634. J Endourol. 2005. PMID: 16053351 Review.
-
Laparoscopic and partial nephrectomy.Clin Cancer Res. 2004 Sep 15;10(18 Pt 2):6322S-7S. doi: 10.1158/1078-0432.CCR-050003. Clin Cancer Res. 2004. PMID: 15448025 Review.
References
-
- Srinualnad S, Mahawong P. Conventional laparoscopic partial nephrectomy for a small renalmass. J Med Assoc Thai (2007) 90(6):1225–30. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials