

Platelet-to-Lymphocyte Ratio (PLR) as the Prognostic Factor for Recurrence/Residual Disease in HSIL Patients After LEEP
- PMID: 37152868
- PMCID: PMC10162391
- DOI: 10.2147/JIR.S406082
Platelet-to-Lymphocyte Ratio (PLR) as the Prognostic Factor for Recurrence/Residual Disease in HSIL Patients After LEEP
Abstract
Purpose: The platelet-to-lymphocyte ratio (PLR) is considered correlated with cancer prognosis including cervical cancer, in addition to high-risk papillomavirus (HR-HPV) infection, of which the predictive value in prognosis of high-grade squamous intraepithelial lesions (HSILs) remains unknown. Here, the prognostic predictive value of PLR in HSIL after loop electrosurgical excision procedure (LEEP) was evaluated.
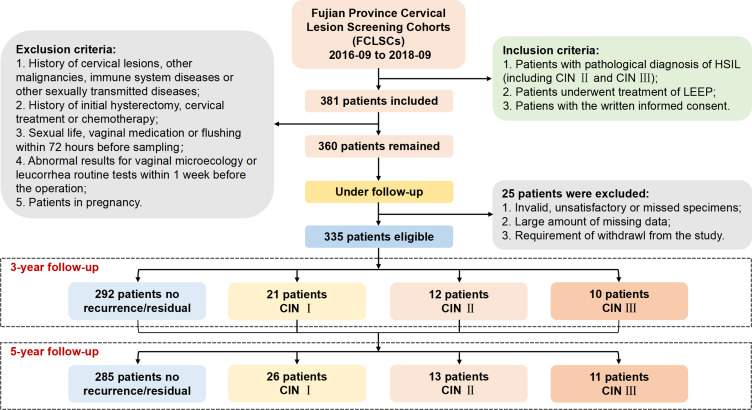
Patients and methods: This study included 335 nonpregnant participants with histopathologically confirmed HSIL and 3- and 5-year follow-ups from the Fujian Cervical Lesions Screening Cohorts (FCLSCs) between September 2016 and September 2018. PLR and other variables were evaluated to identify the factors related to the recurrence/residual cervical intraepithelial neoplasia (CIN)-free survival (RFS), namely, the time from LEEP at baseline to first detection of recurrence/residual CIN or end of follow-up, by logistic and Cox regression.
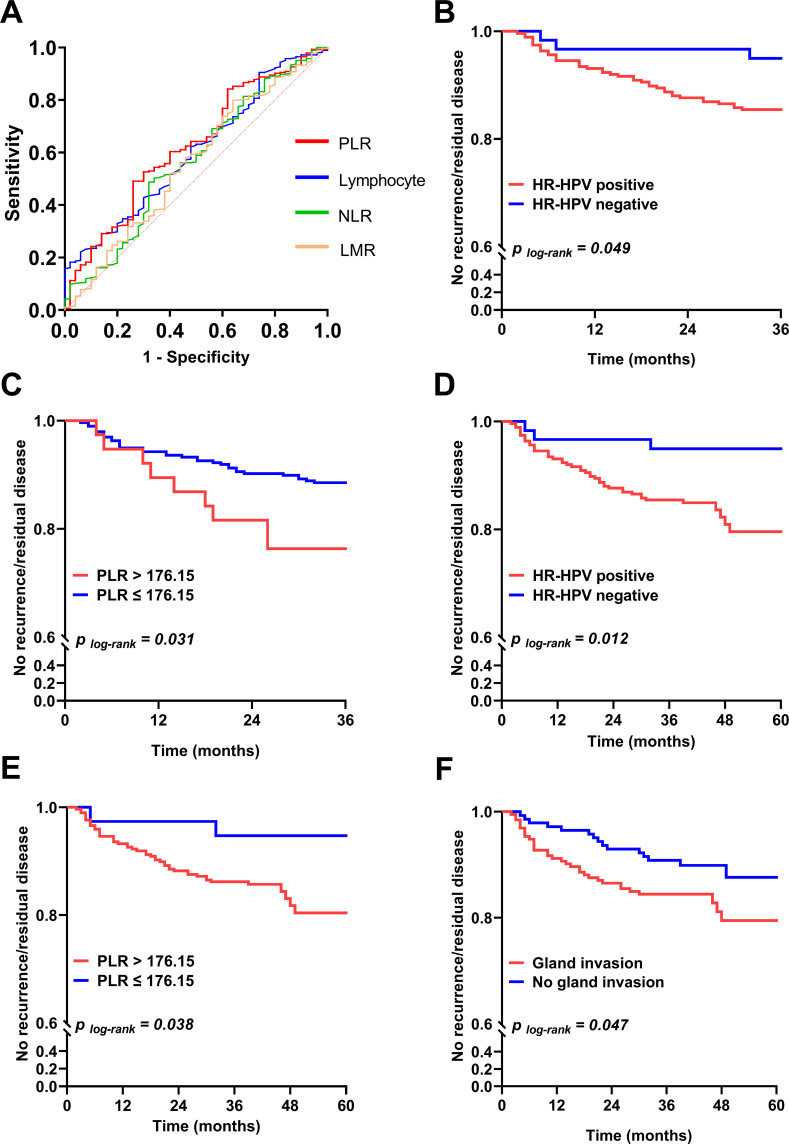
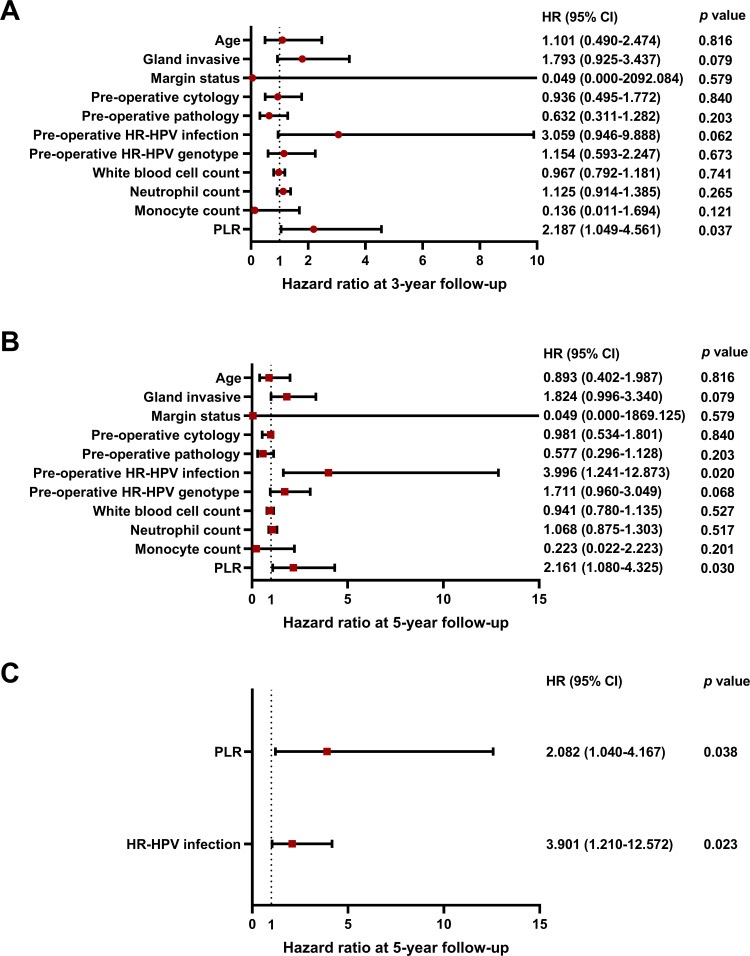
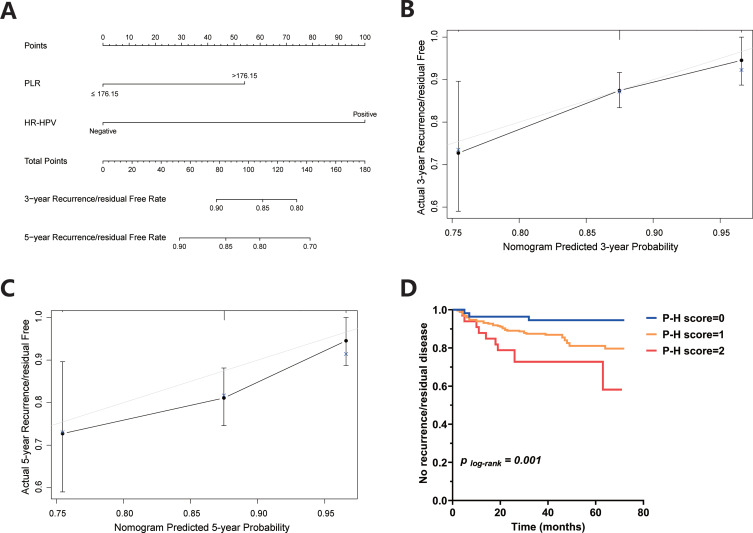
Results: In the Kaplan‒Meier analysis, HR-HPV infection (p=0.049/0.012), higher PLR (p=0.031/0.038), and gland invasion (p=0.047) had a higher risk for recurrence/residual CIN at the 3-/5-year follow-up. The univariate logistic and Cox regression analyses showed significant differences and a higher cumulative risk in patients with HR-HPV infection (OR=3.917, p=0.026; HR=3.996, p=0.020) and higher PLR (OR=2.295, p=0.041; HR=2.161, p=0.030) at the 5-year follow-up. The findings by multivariate Cox regression analysis were similar, indicating a poor prognosis for patients with HR-HPV infection (HR=3.901, p=0.023) and higher PLR (HR=2.082, p=0.038) at the 5-year follow-up. The calibration plot showed a better model fit for RFS at the 3-year follow-up.
Conclusion: Preoperative PLR level and HR-HPV infection could be available markers for predicting recurrence/residual disease of HSIL after LEEP. Clinically, combining PLR with HR-HPV tests may provide novel evaluation method and reference for management in post-treatment patients with cervical precancerous lesions.
Keywords: HPV; cervical intraepithelial neoplasia; conization; human papillomavirus; prognosis; systemic inflammatory response.
© 2023 Huang et al.
Conflict of interest statement
No potential conflict of interest relevant to this article was declared.
Figures
Similar articles
-
Prognostic Prediction for Recurrent/Residual CIN in HSIL Patients After Conization: An Updated Retrospective Study Based on Ambulatory Surgery.J Inflamm Res. 2024 Nov 19;17:9087-9102. doi: 10.2147/JIR.S494622. eCollection 2024. J Inflamm Res. 2024. PMID: 39583852 Free PMC article.
-
[Clinical outcome and high risk factor for residual lesion analysis of HSIL half a year after loop electrosurgical excision procedure: a clinical study of 1 502 cases].Zhonghua Fu Chan Ke Za Zhi. 2017 Nov 25;52(11):751-756. doi: 10.3760/cma.j.issn.0529-567X.2017.11.007. Zhonghua Fu Chan Ke Za Zhi. 2017. PMID: 29179270 Chinese.
-
Analysis of serum NLR combined with intraoperative margin condition to predict the prognosis of cervical HSIL patients undergoing LEEP surgery.Open Med (Wars). 2025 Mar 6;20(1):20241101. doi: 10.1515/med-2024-1101. eCollection 2025. Open Med (Wars). 2025. PMID: 40061832 Free PMC article.
-
Can Adjuvant HPV Vaccination Be Helpful in the Prevention of Persistent/Recurrent Cervical Dysplasia after Surgical Treatment?-A Literature Review.Cancers (Basel). 2022 Sep 7;14(18):4352. doi: 10.3390/cancers14184352. Cancers (Basel). 2022. PMID: 36139514 Free PMC article. Review.
-
Can prophylactic HPV vaccination reduce the recurrence of cervical lesions after surgery? Review and prospect.Infect Agent Cancer. 2023 Oct 29;18(1):66. doi: 10.1186/s13027-023-00547-2. Infect Agent Cancer. 2023. PMID: 37898754 Free PMC article. Review.
Cited by
-
The Platelet-to-Lymphocyte Ratio (PLR) as a Non-Invasive Biomarker for Cervical Malignancy in Conization Patients.Life (Basel). 2025 Jun 18;15(6):971. doi: 10.3390/life15060971. Life (Basel). 2025. PMID: 40566623 Free PMC article.
-
A predictive model for residual lesions after LEEP surgery in CIN III patients.Front Med (Lausanne). 2023 Dec 11;10:1326833. doi: 10.3389/fmed.2023.1326833. eCollection 2023. Front Med (Lausanne). 2023. PMID: 38148909 Free PMC article.
-
Trends in incidence and mortality for gynaecological cancers in Southeastern China during 2011-2020: a retrospective analysis of registry data.BMJ Open. 2024 Sep 28;14(9):e083336. doi: 10.1136/bmjopen-2023-083336. BMJ Open. 2024. PMID: 39343456 Free PMC article.
-
Inflammatory Markers in Prior Loop Electrosurgical Excision Procedure (LEEP) as a Prognosis Factor in the Recurrence of Cervical Intraepithelial Neoplasia.Asian Pac J Cancer Prev. 2024 May 1;25(5):1635-1641. doi: 10.31557/APJCP.2024.25.5.1635. Asian Pac J Cancer Prev. 2024. PMID: 38809635 Free PMC article.
-
Prognostic Value of Systemic Inflammatory Response Markers for CIN2+ Recurrence After Loop Electrosurgical Excision Procedure: A Retrospective Cohort Study.J Clin Med. 2025 Jun 8;14(12):4059. doi: 10.3390/jcm14124059. J Clin Med. 2025. PMID: 40565805 Free PMC article.
References
LinkOut - more resources
Full Text Sources
