

Germline multigene panel testing of patients with endometrial cancer
- PMID: 37153042
- PMCID: PMC10157349
- DOI: 10.3892/ol.2023.13802
Germline multigene panel testing of patients with endometrial cancer
Abstract
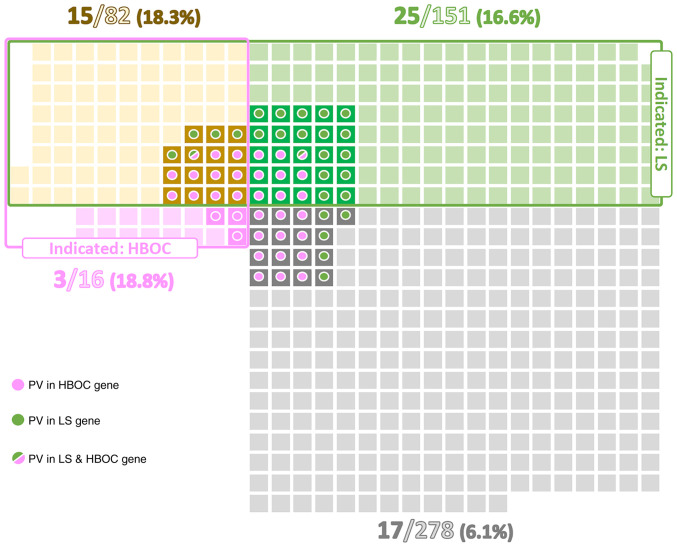
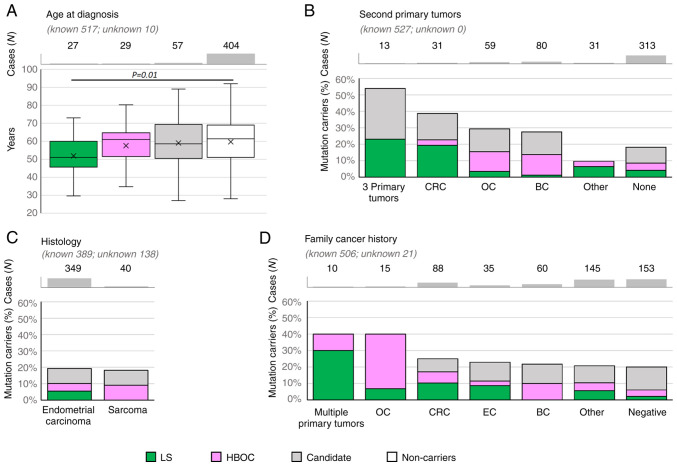
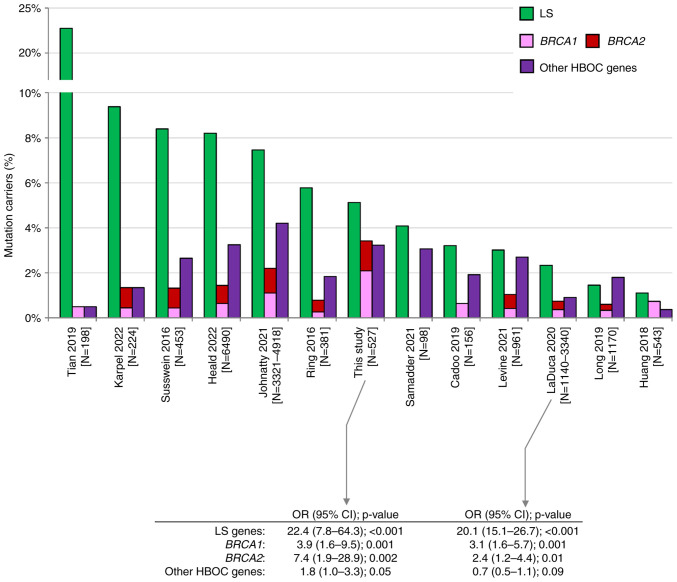
Endometrial cancer (EC) is the most common gynecological malignancy in developed countries. The present study aimed to determine the frequency of germline pathogenic variants (PV) in patients with EC. In this multicenter retrospective cohort study, germline genetic testing (GGT) was performed in 527 patients with EC using a next generation sequencing panel targeting 226 genes, including 5 Lynch syndrome (LS) and 14 hereditary breast and ovarian cancer (HBOC) predisposition genes, and 207 candidate predisposition genes. Gene-level risks were calculated using 1,662 population-matched controls (PMCs). Patients were sub-categorized to fulfill GGT criteria for LS, HBOC, both or none. A total of 60 patients (11.4%) carried PV in LS (5.1%) and HBOC (6.6%) predisposition genes, including two carriers of double PV. PV in LS genes conferred a significantly higher EC risk [odds ratio (OR), 22.4; 95% CI, 7.8-64.3; P=1.8×10-17] than the most frequently altered HBOC genes BRCA1 (OR, 3.9; 95% CI, 1.6-9.5; P=0.001), BRCA2 (OR, 7.4; 95% CI, 1.9-28.9; P=0.002) and CHEK2 (OR, 3.2; 95% CI, 1.0-9.9; P=0.04). Furthermore, >6% of patients with EC not fulfilling LS or HBOC GGT indication criteria carried a PV in a clinically relevant gene. Carriers of PV in LS genes had a significantly lower age of EC onset than non-carriers (P=0.01). Another 11.0% of patients carried PV in a candidate gene (the most frequent were FANCA and MUTYH); however, their individual frequencies did not differ from PMCs (except for aggregated frequency of loss-of-function variants in POLE/POLD1; OR, 10.44; 95% CI, 1.1-100.5; P=0.012). The present study demonstrated the importance of GGT in patients with EC. The increased risk of EC of PV carriers in HBOC genes suggests that the diagnosis of EC should be included in the HBOC GGT criteria.
Keywords: EC; germline mutations; multigene panel testing; uterine malignancies.
Copyright: © Kral et al.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous