

Associations of longitudinal height and weight with clinical outcomes in pediatric kidney replacement therapy: results from the ESPN/ERA Registry
- PMID: 37154961
- PMCID: PMC10465625
- DOI: 10.1007/s00467-023-05973-3
Associations of longitudinal height and weight with clinical outcomes in pediatric kidney replacement therapy: results from the ESPN/ERA Registry
Abstract
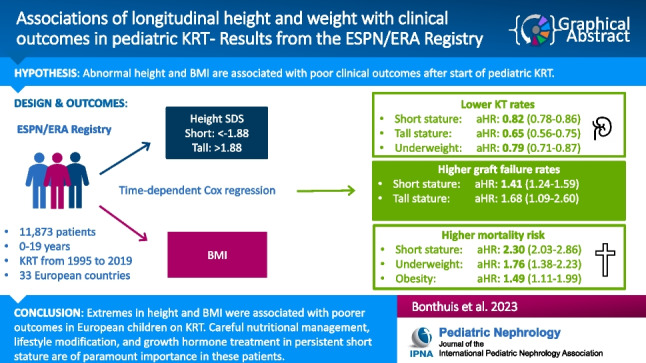
Background: Associations between anthropometric measures and patient outcomes in children are inconsistent and mainly based on data at kidney replacement therapy (KRT) initiation. We studied associations of height and body mass index (BMI) with access to kidney transplantation, graft failure, and death during childhood KRT.
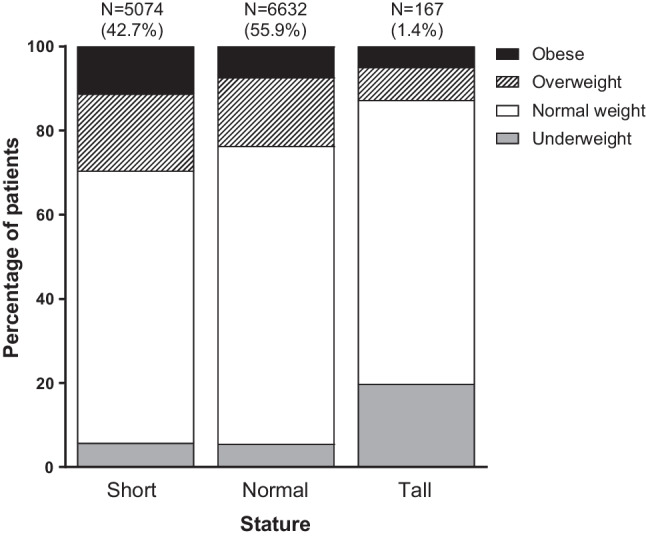
Methods: We included patients < 20 years starting KRT in 33 European countries from 1995-2019 with height and weight data recorded to the ESPN/ERA Registry. We defined short stature as height standard deviation scores (SDS) < -1.88 and tall stature as height SDS > 1.88. Underweight, overweight and obesity were calculated using age and sex-specific BMI for height-age criteria. Associations with outcomes were assessed using multivariable Cox models with time-dependent covariates.
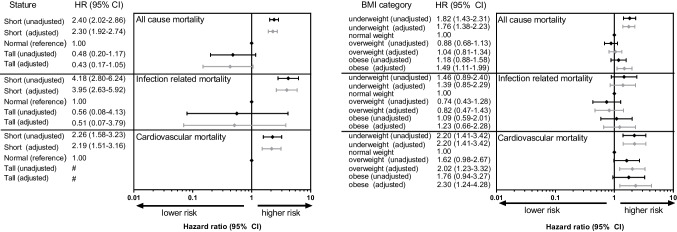
Results: We included 11,873 patients. Likelihood of transplantation was lower for short (aHR: 0.82, 95% CI: 0.78-0.86), tall (aHR: 0.65, 95% CI: 0.56-0.75), and underweight patients (aHR: 0.79, 95%CI: 0.71-0.87). Compared with normal height, patients with short and tall statures showed higher graft failure risk. All-cause mortality risk was higher in short (aHR: 2.30, 95% CI: 1.92-2.74), but not in tall stature. Underweight (aHR: 1.76, 95% CI: 1.38-2.23) and obese (aHR: 1.49, 95% CI: 1.11-1.99) patients showed higher all-cause mortality risk than normal weight subjects.
Conclusions: Short and tall stature and being underweight were associated with a lower likelihood of receiving a kidney allograft. Mortality risk was higher among pediatric KRT patients with a short stature or those being underweight or obese. Our results highlight the need for careful nutritional management and multidisciplinary approach for these patients. A higher resolution version of the Graphical abstract is available as Supplementary information.
Keywords: Body composition; Children; Growth; Kidney transplantation; Mortality.
© 2023. The Author(s).
Conflict of interest statement
We have no conflicts of interest to declare. The results presented in this paper have not been published previously in whole or part, except in abstract form.
Figures
Comment in
-
Anthropometric measures and patient outcome in pediatric chronic kidney disease.Pediatr Nephrol. 2023 Oct;38(10):3207-3210. doi: 10.1007/s00467-023-06017-6. Epub 2023 May 18. Pediatr Nephrol. 2023. PMID: 37199813 No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
