

Excess Mortality Among Patients in the Veterans Affairs Health System Compared With the Overall US Population During the First Year of the COVID-19 Pandemic
- PMID: 37155169
- PMCID: PMC10167568
- DOI: 10.1001/jamanetworkopen.2023.12140
Excess Mortality Among Patients in the Veterans Affairs Health System Compared With the Overall US Population During the First Year of the COVID-19 Pandemic
Abstract
Importance: During the first year of the COVID-19 pandemic, there was a substantial increase in the rate of death in the United States. It is unclear whether those who had access to comprehensive medical care through the Department of Veterans Affairs (VA) health care system had different death rates compared with the overall US population.
Objective: To quantify and compare the increase in death rates during the first year of the COVID-19 pandemic between individuals who received comprehensive medical care through the VA health care system and those in the general US population.
Design, setting, and participants: This cohort study compared 10.9 million enrollees in the VA, including 6.8 million active users of VA health care (those with a visit in the last 2 years), with the general population of the US, with deaths occurring from January 1, 2014, to December 31, 2020. Statistical analysis was conducted from May 17, 2021, to March 15, 2023.
Main outcomes and measures: Changes in rates of death from any cause during the COVID-19 pandemic in 2020 compared with previous years. Changes in all-cause death rates by quarter were stratified by age, sex, race and ethnicity, and region, based on individual-level data. Multilevel regression models were fit in a bayesian setting. Standardized rates were used for comparison between populations.
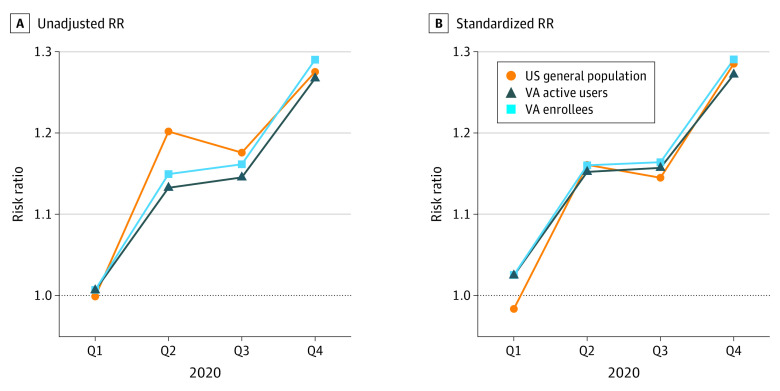
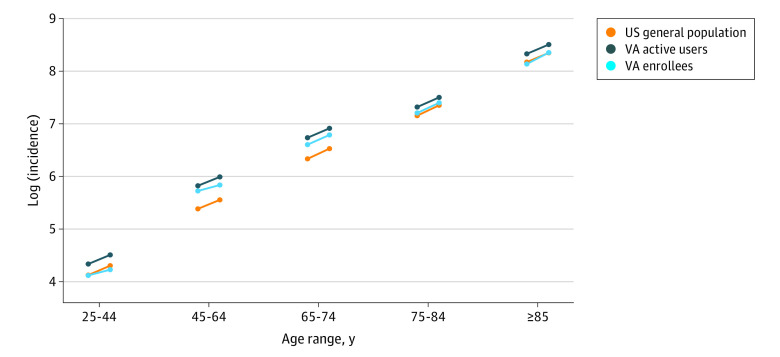
Results: There were 10.9 million enrollees in the VA health care system and 6.8 million active users. The demographic characteristics of the VA populations were predominantly male (>85% in the VA health care system vs 49% in the general US population), older (mean [SD], 61.0 [18.2] years in the VA health care system vs 39.0 [23.1] years in the US population), and had a larger proportion of patients who were White (73% in the VA health care system vs 61% in the US population) or Black (17% in the VA health care system vs 13% in the US population). Increases in death rates were apparent across all of the adult age groups (≥25 years) in both the VA populations and the general US population. Across all of 2020, the relative increase in death rates compared with expected values was similar for VA enrollees (risk ratio [RR], 1.20 [95% CI, 1.14-1.29]), VA active users (RR, 1.19 [95% CI, 1.14-1.26]), and the general US population (RR, 1.20 [95% CI, 1.17-1.22]). Because the prepandemic standardized mortality rates were higher in the VA populations prior to the pandemic, the absolute rates of excess mortality were higher in the VA populations.
Conclusions and relevance: In this cohort study, a comparison of excess deaths between populations suggests that active users of the VA health system had similar relative increases in mortality compared with the general US population during the first 10 months of the COVID-19 pandemic.
Conflict of interest statement
Figures
Similar articles
-
Risk Factors for Hospitalization, Mechanical Ventilation, or Death Among 10 131 US Veterans With SARS-CoV-2 Infection.JAMA Netw Open. 2020 Sep 1;3(9):e2022310. doi: 10.1001/jamanetworkopen.2020.22310. JAMA Netw Open. 2020. PMID: 32965502 Free PMC article.
-
Rates of Primary Care and Integrated Mental Health Telemedicine Visits Between Rural and Urban Veterans Affairs Beneficiaries Before and After the Onset of the COVID-19 Pandemic.JAMA Netw Open. 2023 Mar 1;6(3):e231864. doi: 10.1001/jamanetworkopen.2023.1864. JAMA Netw Open. 2023. PMID: 36881410 Free PMC article.
-
Association of Social and Behavioral Risk Factors With Mortality Among US Veterans With COVID-19.JAMA Netw Open. 2021 Jun 1;4(6):e2113031. doi: 10.1001/jamanetworkopen.2021.13031. JAMA Netw Open. 2021. PMID: 34106264 Free PMC article.
-
Characteristics and Health Care Expenditures of VA Health System Users versus Other Veterans, 2014-2015 (Combined).2018 Jan. In: Statistical Brief (Medical Expenditure Panel Survey (US)) [Internet]. Rockville (MD): Agency for Healthcare Research and Quality (US); 2001–. STATISTICAL BRIEF #508. 2018 Jan. In: Statistical Brief (Medical Expenditure Panel Survey (US)) [Internet]. Rockville (MD): Agency for Healthcare Research and Quality (US); 2001–. STATISTICAL BRIEF #508. PMID: 29369580 Free Books & Documents. Review.
-
Risk and Protective Factors Across Socioecological Levels of Risk for Suicide: An Evidence Map [Internet].Washington (DC): Department of Veterans Affairs (US); 2021 Aug. Washington (DC): Department of Veterans Affairs (US); 2021 Aug. PMID: 34846828 Free Books & Documents. Review.
Cited by
-
Impact of the COVID-19 Pandemic on the Provision of Dialysis Service and Mortality in Veterans Receiving Maintenance Hemodialysis in the VA: An Interrupted Time-Series Analysis.Am J Nephrol. 2023;54(11-12):508-515. doi: 10.1159/000532105. Epub 2023 Jul 31. Am J Nephrol. 2023. PMID: 37524062 Free PMC article.
-
Veteran Preferences and Willingness to Share Patient-Generated Health Data.J Gen Intern Med. 2025 Apr;40(5):1157-1165. doi: 10.1007/s11606-024-09095-w. Epub 2024 Oct 16. J Gen Intern Med. 2025. PMID: 39414734
-
Early effectiveness of the BNT162b2 KP.2 vaccine against COVID-19 in the US Veterans Affairs Healthcare System.Nat Commun. 2025 Apr 29;16(1):4033. doi: 10.1038/s41467-025-59344-7. Nat Commun. 2025. PMID: 40301395 Free PMC article.
-
Excess mortality in US Veterans during the COVID-19 pandemic: an individual-level cohort study.Int J Epidemiol. 2023 Dec 25;52(6):1725-1734. doi: 10.1093/ije/dyad136. Int J Epidemiol. 2023. PMID: 37802889 Free PMC article.
-
Outpatient care changes and associated mortality among Veterans with heart failure during the COVID-19 pandemic.PLoS One. 2025 May 16;20(5):e0323308. doi: 10.1371/journal.pone.0323308. eCollection 2025. PLoS One. 2025. PMID: 40378140 Free PMC article.
References
-
- Lee W-E, Park SW, Weinberger DM, et al. . Direct and indirect mortality impacts of the COVID-19 pandemic in the US, March 2020-April 2021. medRxiv. Preprint posted online February 15, 2022. doi:10.1101/2022.02.10.22270721 - DOI
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
