

Primary Occurrence of Cardiovascular Events After Adding Sodium-Glucose Cotransporter-2 Inhibitors or Glucagon-like Peptide-1 Receptor Agonists Compared With Dipeptidyl Peptidase-4 Inhibitors: A Cohort Study in Veterans With Diabetes
- PMID: 37155984
- PMCID: PMC10367222
- DOI: 10.7326/M22-2751
Primary Occurrence of Cardiovascular Events After Adding Sodium-Glucose Cotransporter-2 Inhibitors or Glucagon-like Peptide-1 Receptor Agonists Compared With Dipeptidyl Peptidase-4 Inhibitors: A Cohort Study in Veterans With Diabetes
Abstract
Background: The effectiveness of glucagon-like peptide-1 receptor agonists (GLP1RA) and sodium-glucose cotransporter-2 inhibitors (SGLT2i) in preventing major adverse cardiac events (MACE) is uncertain for those without preexisting cardiovascular disease.
Objective: To test the hypothesis that MACE incidence was lower with the addition of GLP1RA or SGLT2i compared with dipeptidyl peptidase-4 inhibitors (DPP4i) for primary cardiovascular prevention.
Design: Retrospective cohort study of U.S. veterans from 2001 to 2019.
Setting: Veterans aged 18 years or older receiving care from the Veterans Health Administration, with data linkage to Medicare, Medicaid, and the National Death Index.
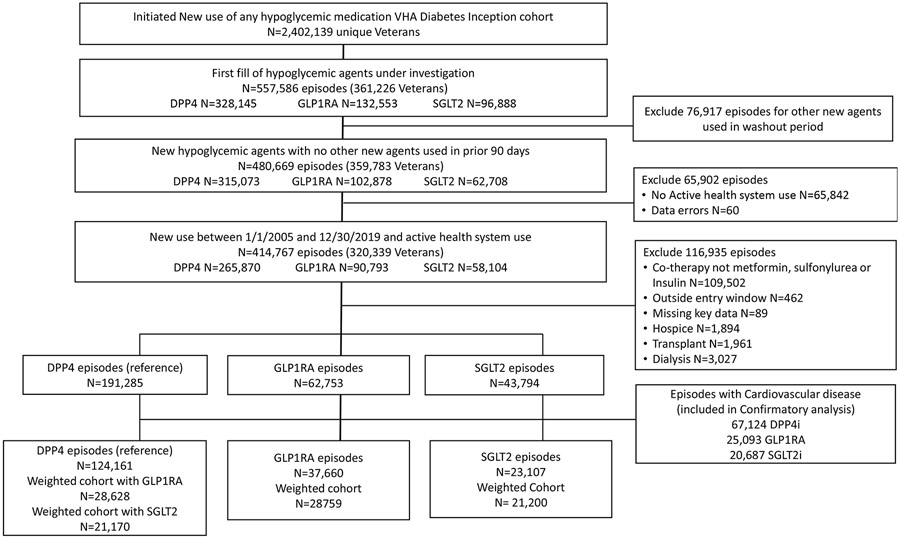
Patients: Veterans adding GLP1RA, SGLT2i, or DPP4i onto metformin, sulfonylurea, or insulin treatment alone or in combination. Episodes were stratified by history of cardiovascular disease.
Measurements: Study outcomes were MACE (acute myocardial infarction, stroke, or cardiovascular death) and heart failure (HF) hospitalization. Cox models compared the outcome between medication groups using pairwise comparisons in a weighted cohort adjusted for covariates.
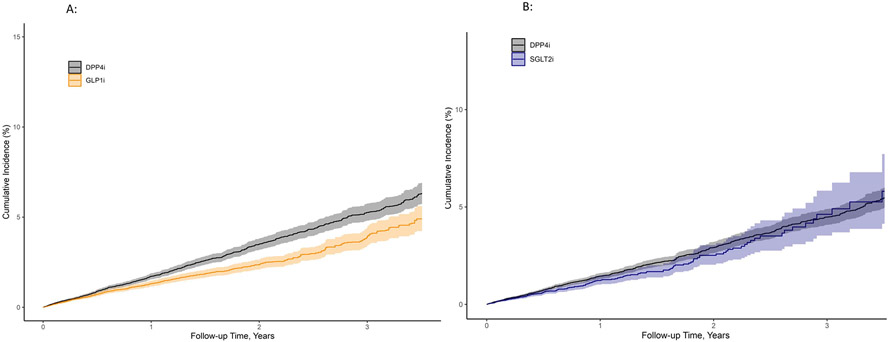
Results: The cohort included 28 759 GLP1RA versus 28 628 DPP4i weighted pairs and 21 200 SGLT2i versus 21 170 DPP4i weighted pairs. Median age was 67 years, and diabetes duration was 8.5 years. Glucagon-like peptide-1 receptor agonists were associated with lower MACE and HF versus DPP4i (adjusted hazard ratio [aHR], 0.82 [95% CI, 0.72 to 0.94]), yielding an adjusted risk difference (aRD) of 3.2 events (CI, 1.1 to 5.0) per 1000 person-years. Sodium-glucose cotransporter-2 inhibitors were not associated with MACE and HF (aHR, 0.91 [CI, 0.78 to 1.08]; aRD, 1.28 [-1.12 to 3.32]) compared with DPP4i.
Limitation: Residual confounding; use of DPP4i, GLP1RA, and SGLT2i as first-line therapies were not examined.
Conclusion: The addition of GLP1RA was associated with primary reductions of MACE and HF hospitalization compared with DPP4i use; SGLT2i addition was not associated with primary MACE prevention.
Primary funding source: VA Clinical Science Research and Development and supported in part by the Centers for Diabetes Translation Research.
Conflict of interest statement
Figures
References
-
- Joseph JJ, Deedwania P, Acharya T, Aguilar D, Bhatt DL, Chyun DA, et al. Comprehensive Management of Cardiovascular Risk Factors for Adults With Type 2 Diabetes: A Scientific Statement From the American Heart Association. Circulation. 2022. Mar;145(9):e722–59. - PubMed
-
- Grundy SM, Benjamin IJ, Burke GL, Chait A, Eckel RH, Howard BV, et al. Diabetes and Cardiovascular Disease. Circulation. 1999. Sep 7;100(10):1134–46. - PubMed
-
- Green JB, Bethel MA, Armstrong PW, Buse JB, Engel SS, Garg J, et al. Effect of Sitagliptin on Cardiovascular Outcomes in Type 2 Diabetes. N Engl J Med. 2015. Jul 16;373(3):232–42. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous