

Influence of surgical margin width on survival rate after resection of intrahepatic cholangiocarcinoma: a systematic review and meta-analysis
- PMID: 37156579
- PMCID: PMC10174020
- DOI: 10.1136/bmjopen-2022-067222
Influence of surgical margin width on survival rate after resection of intrahepatic cholangiocarcinoma: a systematic review and meta-analysis
Abstract
Objectives: Hepatectomy is the best treatment for patients with intrahepatic cholangiocarcinoma (ICC) at present, but there has been controversy about the width of surgical margins. In this study, we systematically investigated the effects of different surgical margin widths on the prognosis of patients with ICC undergoing hepatectomy.
Design: Systematic review and meta-analysis.
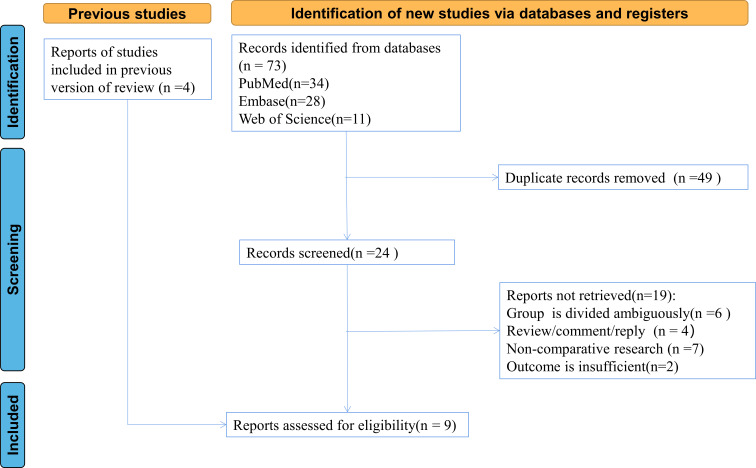
Data sources: PubMed, Embase and Web of Science databases were systematically searched from inception to June 2022.
Eligibility criteria: Cohort studies reported in English with patients who underwent negative marginal (R0) resection were included. The effects of surgical margin width on overall survival (OS), disease-free survival (DFS) and recurrence-free survival (RFS) in patients with ICC were assessed.
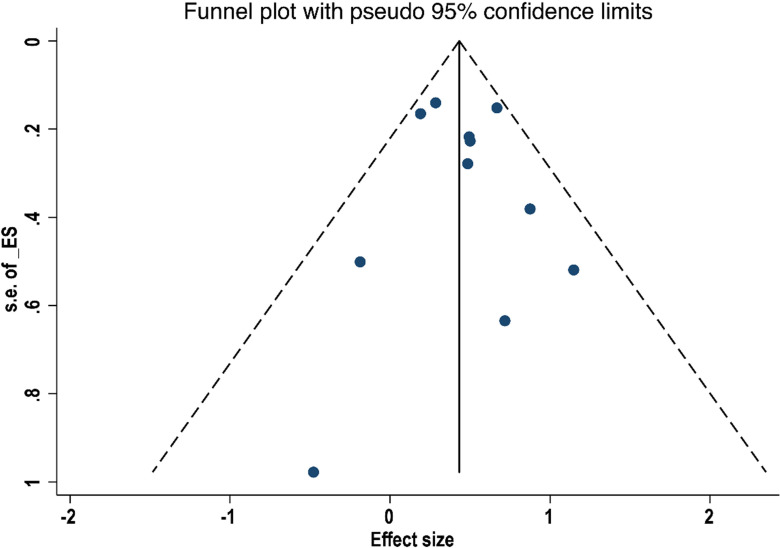
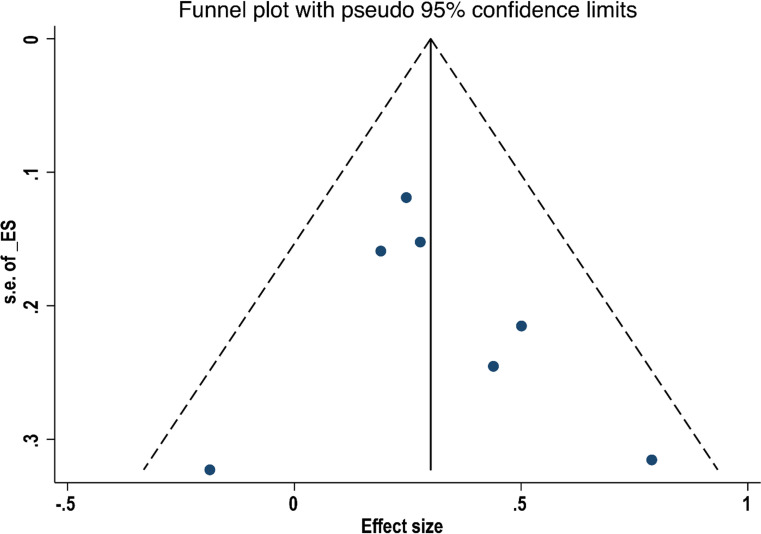
Data extraction and synthesis: Two investigators independently conducted literature screening and data extraction. Risk of bias was assessed using funnel plots and quality was assessed by the Newcastle-Ottawa Scale. Forest plots of HRs and their 95% CIs for outcome indicators were plotted. Heterogeneity was assessed and determined quantitatively using I2, and the stability of the study results was evaluated using sensitivity analysis. Analyses were performed using Stata software.
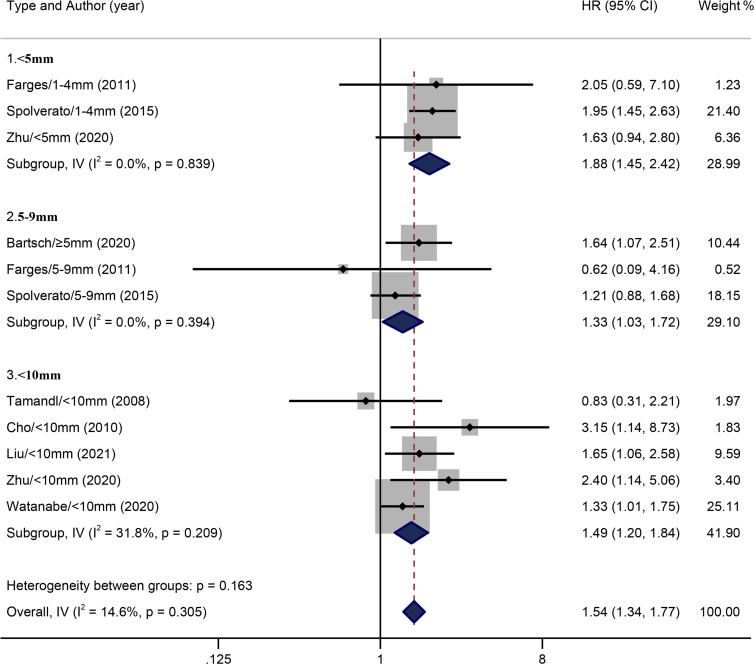
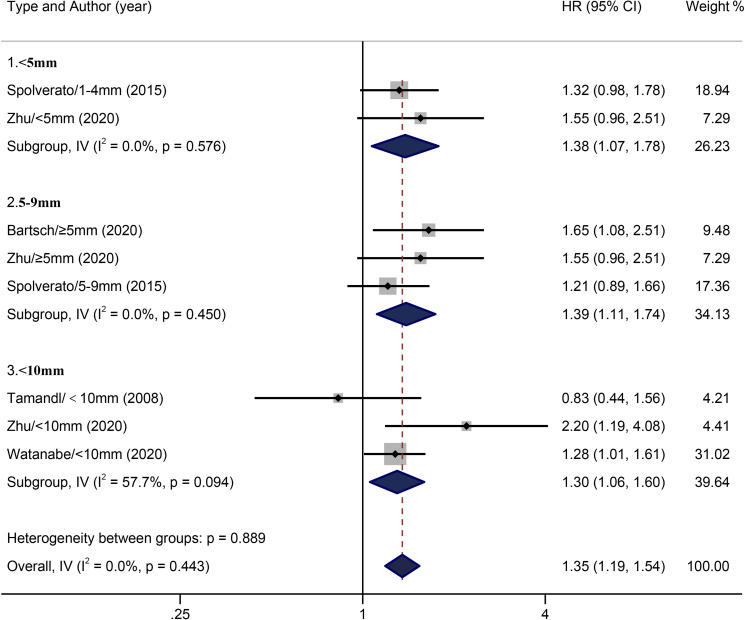
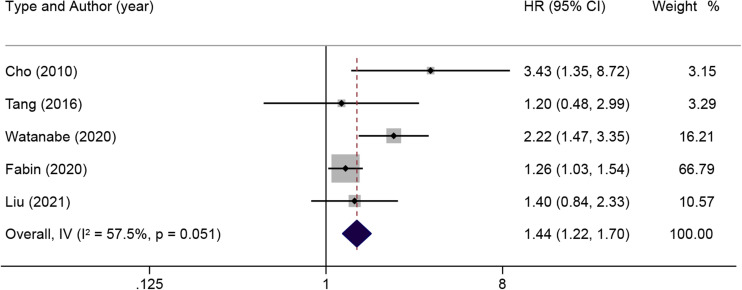
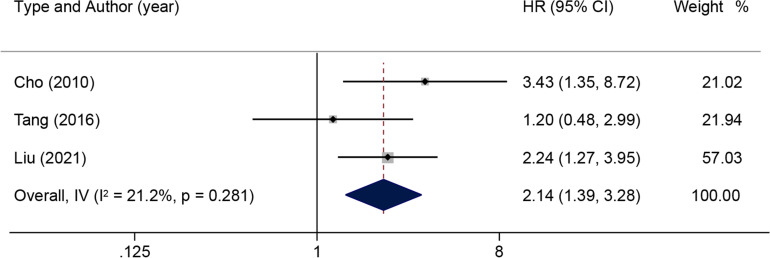
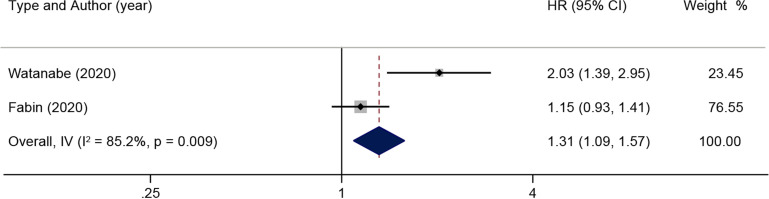
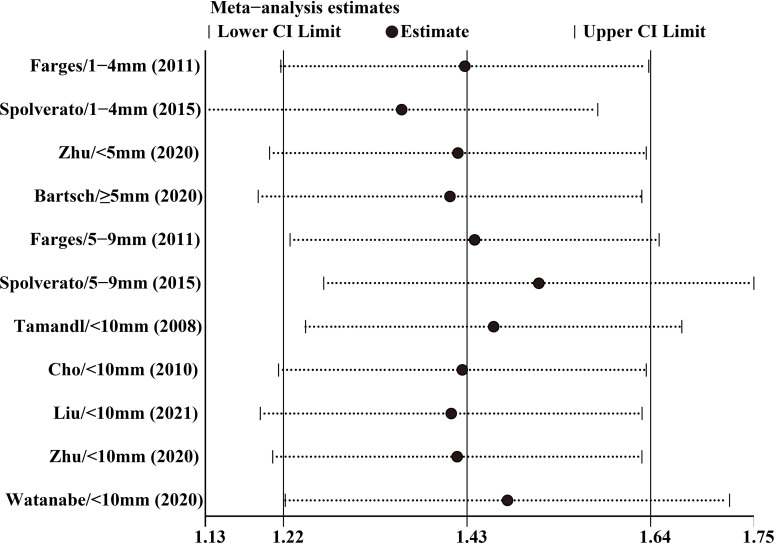
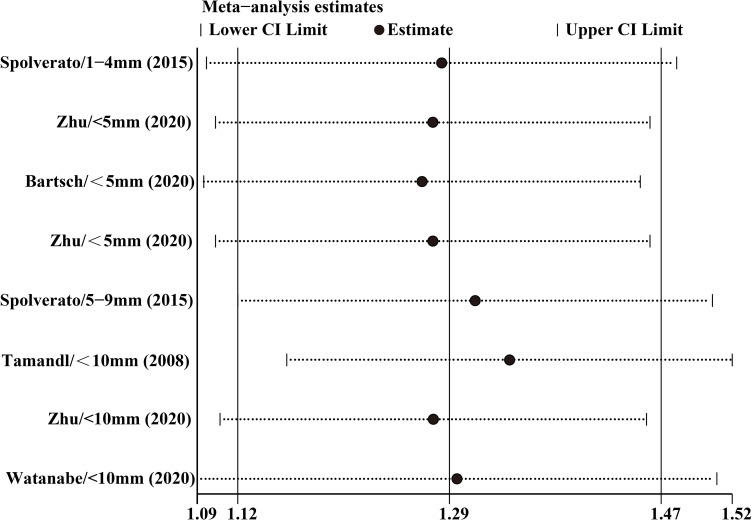
Results: Nine studies were included. With the wide margin group (≥10 mm) as the control, pooled HR of OS in the narrow margin group (<10 mm) was 1.54 (95% CI 1.34 to 1.77). HRs of OS in three subgroups where the margin was less than 5 mm ranged from 5 mm to 9 mm, or was less than 10 mm in length were 1.88 (1.45 to 2.42), 1.33 (1.03 to 1.72) and 1.49 (1.20 to 1.84), respectively. Pooled HR of DFS in the narrow margin group (<10 mm) was 1.51 (1.14 to 2.00). Pooled HR of RFS in the narrow margin group (<10 mm) was 1.35 (1.19 to 1.54). HRs of RFS in three subgroups where the margin was less than 5 mm ranged from 5 mm to 9 mm, or was less than 10 mm in length were 1.38 (1.07 to 1.78), 1.39 (1.11 to 1.74) and 1.30 (1.06 to 1.60), respectively. Neither lymph node lesions (HR 1.44, 95% CI 1.22 to 1.70) nor lymph node invasion (2.14, 1.39 to 3.28) was favourable for postoperative OS in patients with ICC. Lymph node metastasis (1.31, 1.09 to 1.57) was unfavourable for RFS in patients with ICC.
Conclusion: Patients with ICC who underwent curative hepatectomy with a negative margin ≥10 mm may have a long-term survival advantage, but lymph node dissection also needs to be considered. In addition, tumour-related pathological features need to be explored to see if they affect the surgical outcome of R0 margins.
Keywords: Hepatobiliary disease; Hepatobiliary tumours; Hepatology.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures

Similar articles
-
The Application of Artificial Intelligence to Investigate Long-Term Outcomes and Assess Optimal Margin Width in Hepatectomy for Intrahepatic Cholangiocarcinoma.Ann Surg Oncol. 2023 Jul;30(7):4292-4301. doi: 10.1245/s10434-023-13349-y. Epub 2023 Mar 23. Ann Surg Oncol. 2023. PMID: 36952150
-
Prognostic value of resection margin length after surgical resection for intrahepatic cholangiocarcinoma.Am J Surg. 2021 Aug;222(2):383-389. doi: 10.1016/j.amjsurg.2020.12.022. Epub 2020 Dec 15. Am J Surg. 2021. PMID: 33388133
-
The influence of resection margin width in patients with intrahepatic cholangiocarcinoma: a meta-analysis.World J Surg Oncol. 2023 Jan 20;21(1):16. doi: 10.1186/s12957-023-02901-5. World J Surg Oncol. 2023. PMID: 36658564 Free PMC article. Review.
-
The Impact of Surgical Margin Status on Long-Term Outcome After Resection for Intrahepatic Cholangiocarcinoma.Ann Surg Oncol. 2015 Nov;22(12):4020-8. doi: 10.1245/s10434-015-4472-9. Epub 2015 Mar 12. Ann Surg Oncol. 2015. PMID: 25762481
-
Influence of surgical margins on overall survival after resection of intrahepatic cholangiocarcinoma: A meta-analysis.Medicine (Baltimore). 2016 Aug;95(35):e4621. doi: 10.1097/MD.0000000000004621. Medicine (Baltimore). 2016. PMID: 27583880 Free PMC article. Review.
Cited by
-
The conditional recurrence-free survival after R0 hepatectomy for locally advanced intrahepatic cholangiocarcinoma: A competing risk analysis based on inflammation-nutritional status.Heliyon. 2024 Jul 2;10(13):e33931. doi: 10.1016/j.heliyon.2024.e33931. eCollection 2024 Jul 15. Heliyon. 2024. PMID: 39055818 Free PMC article.
-
Intrahepatic cholangiocarcinoma with extensive intraductal extension of high-grade biliary intraepithelial neoplasia: a case report.Surg Case Rep. 2023 Sep 18;9(1):164. doi: 10.1186/s40792-023-01748-y. Surg Case Rep. 2023. PMID: 37721561 Free PMC article.
-
Preoperative prediction model of microvascular invasion in intrahepatic cholangiocarcinoma patients based on CT radiomics can assist clinical surgical decision-making: a multicenter study.Eur Radiol. 2025 Aug 14. doi: 10.1007/s00330-025-11900-x. Online ahead of print. Eur Radiol. 2025. PMID: 40813506
-
Perihilar and Intrahepatic Cholangiocarcinoma after Resection: Clinicopathological Characteristics, Outcomes, and Implications for Addition of Chemoradiotherapy.Euroasian J Hepatogastroenterol. 2024 Jul-Dec;14(2):134-144. doi: 10.5005/jp-journals-10018-1440. Epub 2024 Dec 27. Euroasian J Hepatogastroenterol. 2024. PMID: 39802851 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical