

Management of the COVID-19 pandemic in Rhineland-Palatinate hospitals of all levels of care : Results of the COVID-19 Registry RLP
- PMID: 37156927
- PMCID: PMC10166456
- DOI: 10.1007/s00059-023-05187-1
Management of the COVID-19 pandemic in Rhineland-Palatinate hospitals of all levels of care : Results of the COVID-19 Registry RLP
Abstract
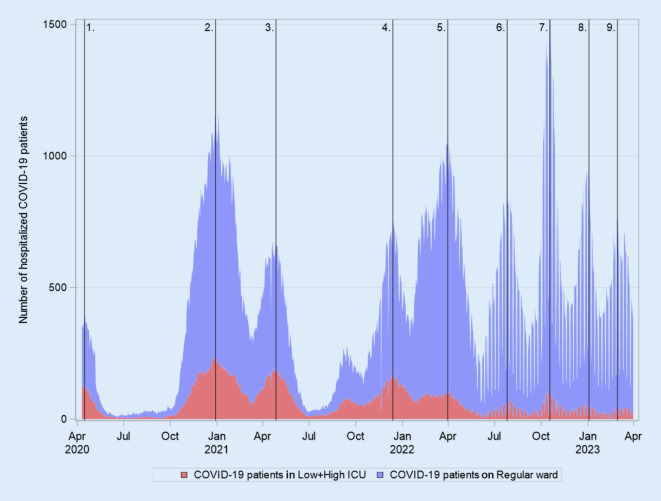
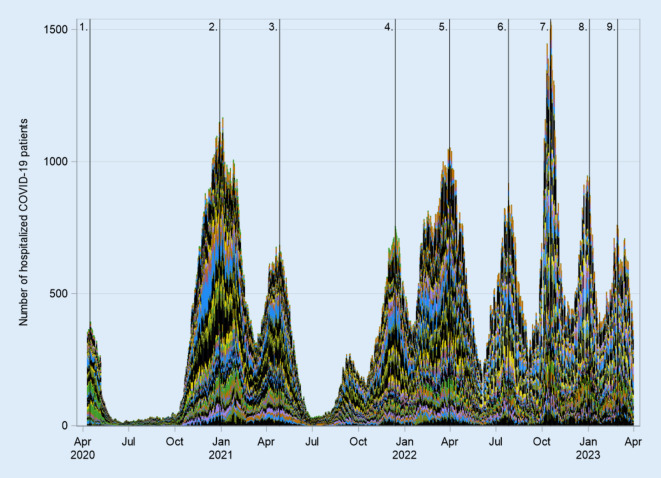
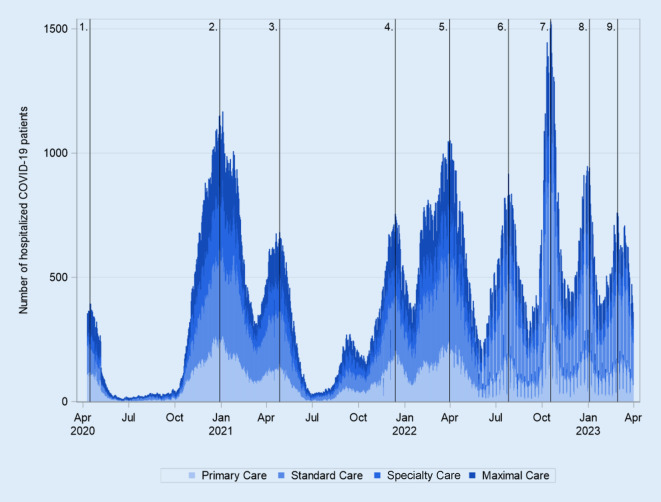
The COVID-19 pandemic placed a significant burden on the German healthcare system. Based on the experience of severe disease progression of the SARS-CoV‑2 infection from neighboring European countries in the early 2020s, with ICU overload and high mortality rates, efforts were made in Germany to increase the capacity of available ICU beds. Subsequently, all documentation and reporting focused on the ICU capacities for COVID-19 patients. It was hypothesized that mainly a few large hospitals provided care for the majority of COVID-19 patients. The COVID-19 Registry RLP of Rhineland-Palatinate documented SARS-CoV‑2 inpatients from daily mandatory queries of all hospitals throughout the pandemic from April 2020 to March 2023, distinguishing between patients in ICUs and normal wards. In its 18th Corona Ordinance, the state government required all hospitals to participate in the care of SARS-CoV‑2 inpatients. We investigated the participation of hospitals at different levels of care in Rhineland-Palatinate in the management of the COVID-19 pandemic. Nine pandemic waves were documented during the pandemic and exemplary data on the respective pandemic peaks were evaluated. A distinction was made between the burden on hospitals at different levels of care: primary care hospitals, standard care hospitals, specialty hospitals, and maximal care hospitals. Analysis of the data showed that all hospital types participated equally in the care of SARS-CoV-2 patients. The requirement of the Ministry of Health of Rhineland-Palatinate to provide at least 20% of the available capacity was met by all levels of care and there were no disparities between hospitals of different levels of care in the management of the pandemic.Hospitals at all levels of care participated equally in the care of SARS-CoV‑2 inpatients and thus contributed significantly to the management of the pandemic in Rhineland-Palatinate.
Die COVID-19-Pandemie stellte eine erhebliche Belastung für das deutsche Gesundheitssystem dar. Aufgrund der Erfahrungen schwerer Krankheitsverläufe der SARS-CoV-2-Infektion aus europäischen Nachbarländern Anfang des Jahres 2020 mit Überlastungen der Intensivstationen und einer hohen Sterblichkeit wurden in Deutschland Anstrengungen unternommen, die Kapazitäten zur Verfügung stehender Intensivbetten zu erhöhen. Sämtliche Dokumentationen sowie die Berichterstattungen konzentrierten sich fortan auf die für die COVID-19-Patienten genutzten und frei verfügbaren Intensivkapazitäten. Dabei wurde wiederholt die Hypothese aufgestellt, dass wenige große Krankenhäuser die Mehrzahl der COVID-19-Patienten versorgt hätten. Das COVID-19-Register des Bundeslandes Rheinland-Pfalz (RLP) hat über die gesamte Pandemiedauer von April 2020 bis März 2023 die stationären SARS-CoV-2-Patienten in täglichen verpflichtenden Abfragen aller Krankenhäuser dokumentiert, differenziert auch zwischen Patienten auf Intensivstationen und Normalstationen. Die Landesregierung hatte in ihrer 18. Corona-Verordnung alle Krankenhäuser zur Beteiligung an der Versorgung der stationären SARS-CoV-2 Patienten verpflichtet. Wir haben die Beteiligung der Krankenhäuser der unterschiedlichen Versorgungsstufen in Rheinland-Pfalz an der Bewältigung der COVID-19-Pandemie untersucht. Es wurden insgesamt 9 Pandemiewellen über den Gesamtzeitraum der Pandemie dokumentiert und exemplarische Daten zu den jeweiligen Pandemieapitzen wurden ausgewertet. Dabei wurde zwischen der Belastung der Krankenhäuser unterschiedlicher Versorgungsstufen unterschieden: Krankenhäuser der Regelversorgung, Krankenhäuser der Grundversorgung, Schwerpunktkrankenhäuser und Krankenhäuser der Maximalversorgung. Die Auswertung der Daten zeigte, dass alle Krankenhaustypen proportional in gleicher Weise an der Versorgung der SARS-CoV-2 Patienten teilgenommen hatten. Die Vorgabe des Gesundheitsministerium von RLP, mindestens 20 % der verfügbaren Kapazitäten zur Verfügung zu stellen, wurde von allen Versorgungsklassen eingehalten, und es gab keine Ungleichverteilungen im Management der Pandemie. Krankenhäuser aller Versorgungsstufen haben gleichermaßen an der Versorgung der stationären SARS-CoV-2-Patienten teilgenommen und damit maßgeblich zum Management der Pandemie in Rheinland-Pfalz beigetragen.
Keywords: Hospital bed capacity; Hospitalization; Inpatients; Intensive care unit; SARS-CoV‑2.
© 2023. The Author(s), under exclusive licence to Springer Medizin Verlag GmbH, ein Teil von Springer Nature.
Conflict of interest statement
A.K. Gitt, M. Horack, S. Schneider, U. Zeymer and R. Zahn declare that they have no competing interests.
Figures
Similar articles
-
Flexibility and Bed Margins of the Community of Madrid's Hospitals during the First Wave of the SARS-CoV-2 Pandemic.Int J Environ Res Public Health. 2021 Mar 28;18(7):3510. doi: 10.3390/ijerph18073510. Int J Environ Res Public Health. 2021. PMID: 33800638 Free PMC article.
-
[Role of university hospitals in Bavaria during the COVID-19 pandemic].Med Klin Intensivmed Notfmed. 2022 May;117(4):305-308. doi: 10.1007/s00063-021-00793-5. Epub 2021 Mar 1. Med Klin Intensivmed Notfmed. 2022. PMID: 33646331 Free PMC article. German.
-
A country-level analysis comparing hospital capacity and utilisation during the first COVID-19 wave across Europe.Health Policy. 2022 May;126(5):373-381. doi: 10.1016/j.healthpol.2021.11.009. Epub 2021 Dec 1. Health Policy. 2022. PMID: 34924210 Free PMC article.
-
[Managing the pandemic-relocation concept for COVID-19 intensive care patients and non-COVID-19 intensive care patients in Baden-Württemberg].Anaesthesist. 2021 Nov;70(11):951-961. doi: 10.1007/s00101-021-00961-4. Epub 2021 Apr 28. Anaesthesist. 2021. PMID: 33909104 Free PMC article. Review. German.
-
[Impact of the COVID-19 pandemic on the care situation in psychiatric hospitals in Germany].Nervenarzt. 2021 Jun;92(6):562-570. doi: 10.1007/s00115-021-01129-6. Epub 2021 May 18. Nervenarzt. 2021. PMID: 34003321 Free PMC article. Review. German.
References
-
- Achtzehnte Corona-Bekämpfungsverordnung Rheinland-Pfalz (18. CoBeLVO) vom 20. März 2021. https://Corona.rlp.de/fileadmin/coroona/210331_18._CoBeLVO_1AEndVO_konso.... Accessed: 5 May 2023
-
- Gitt AK, Lober C, Neumer A, Schneider S, et al. Krankenhäuser an den Grenzen der Versorgung. Dtsch Arztebl. 2022;119(43):A 1846–A 1850.
-
- Gitt AK, Lober C, Bernhardt A, et al. Coronabelastung auf den Normalstationen stärker beachten: Die Fokussierung auf die Intensivmedizin in der COVID-19-Pandemie ist unzureichend für die Beurteilung der Auslastung des Krankenhaussystems. Dtsch Arztebl. 2022;119(6):221–224.
-
- Loos S, Albrecht M, Zich K. Zukunftsfähige Krankenhausversorgung, Simulation und Analyse einer Neustrukturierung der Krankenhausversorgung am Beispiel einer Versorgungsregion in Nordrhein-Westfalen. Bertelsmann; 2019.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
