

Allogeneic hematopoietic stem cell transplantation for NK/T-cell lymphoma: an international collaborative analysis
- PMID: 37157017
- PMCID: PMC10166457
- DOI: 10.1038/s41375-023-01924-x
Allogeneic hematopoietic stem cell transplantation for NK/T-cell lymphoma: an international collaborative analysis
Abstract
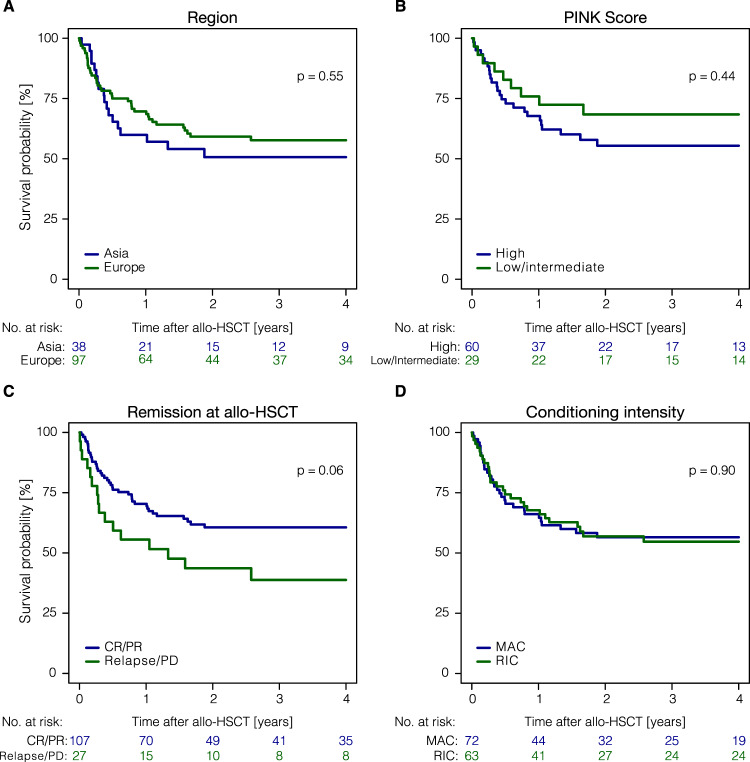
Natural killer/T-cell lymphomas (NKTCL) represent rare and aggressive lymphoid malignancies. Patients (pts) with relapsed/refractory disease after Asparaginase (ASPA)-based chemotherapy have a dismal prognosis. To better define the role of allogeneic hematopoietic stem cell transplantation (allo-HSCT), we conducted a retrospective analysis of data shared with the European Society for Blood and Marrow Transplantation (EBMT) and cooperating Asian centers. We identified 135 pts who received allo-HSCT between 2010 and 2020. Median age was 43.4 years at allo-HSCT, 68.1% were male. Ninety-seven pts (71.9 %) were European, 38 pts (28.1%) Asian. High Prognostic Index for NKTCL (PINK) scores were reported for 44.4%; 76.3% had >1 treatment, 20.7% previous auto-HSCT, and 74.1% ASPA-containing regimens prior to allo-HSCT. Most (79.3%) pts were transplanted in CR/PR. With a median follow-up of 4.8 years, 3-year progression-free(PFS) and overall survival were 48.6% (95%-CI:39.5-57%) and 55.6% (95%-CI:46.5-63.8%). Non-relapse mortality at 1 year was 14.8% (95%-CI:9.3-21.5%) and 1-year relapse incidence 29.6% (95%-CI:21.9-37.6%). In multivariate analyses, shorter time interval (0-12 months) between diagnosis and allo-HSCT [HR = 2.12 (95%-CI:1.03-4.34); P = 0.04] and transplantation not in CR/PR [HR = 2.20 (95%-CI:0.98-4.95); P = 0.056] reduced PFS. Programmed cell death protein 1(PD-1/PD-L1) treatment before HSCT neither increased GVHD nor impacted survival. We demonstrate that allo-HSCT can achieve long-term survival in approximately half of pts allografted for NKTCL.
© 2023. The Author(s).
Conflict of interest statement
HCR received consulting and lecture fees from Abbvie, AstraZeneca, BMS, Roche, Vertex, and Merck. HCR received research funding from Gilead Pharmaceuticals and AstraZeneca. HCR is a co-founder of CDL Therapeutics GmbH. YC received consulting fees from MSD, Novartis, Incyte, BMS, Pfizer, Abbvie, Roche, Jazz, Gilead, Amgen, Astra-Zeneca, Servier; Travel support from MSD, Roche, Gilead, Amgen, Incyte, Abbvie, Janssen, Astra-Zeneca, Jazz. AS received research grants from Takeda, BMS/Celgene. AS received consulting fees from Takeda, BMS/Celgene, Novartis, Janssen, Gilead, and Sanofi. AS received honoraria from Takeda, BMS/Celgene, MSD, Janssen, Amgen, Novartis, Gilead Kite, Sanofi, Roche, and Alexion. The remaining authors declare no competing financial interests.
Figures

References
-
- Kim SJ, Choi JY, Hyun SH, Ki CS, Oh D, Ahn YC, et al. Risk stratification on the basis of Deauville score on PET-CT and the presence of Epstein-Barr virus DNA after completion of primary treatment for extranodal natural killer/T-cell lymphoma, nasal type: a multicentre, retrospective analysis. Lancet Haematol. 2015;2:e66–74. doi: 10.1016/S2352-3026(15)00002-2. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
