

Meniscus Radial Tears: Current Concepts on Management and Repair Techniques
- PMID: 37157051
- PMCID: PMC10188782
- DOI: 10.1007/s12178-023-09831-5
Meniscus Radial Tears: Current Concepts on Management and Repair Techniques
Abstract
Purpose of review: This review provides a historical perspective on the approach to radial tears and collates the currently available evidence on repair techniques, rehabilitation, and outcomes following the treatment of meniscus radial tears.
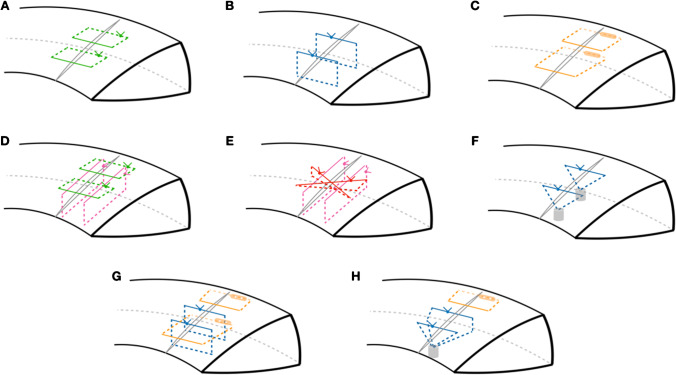
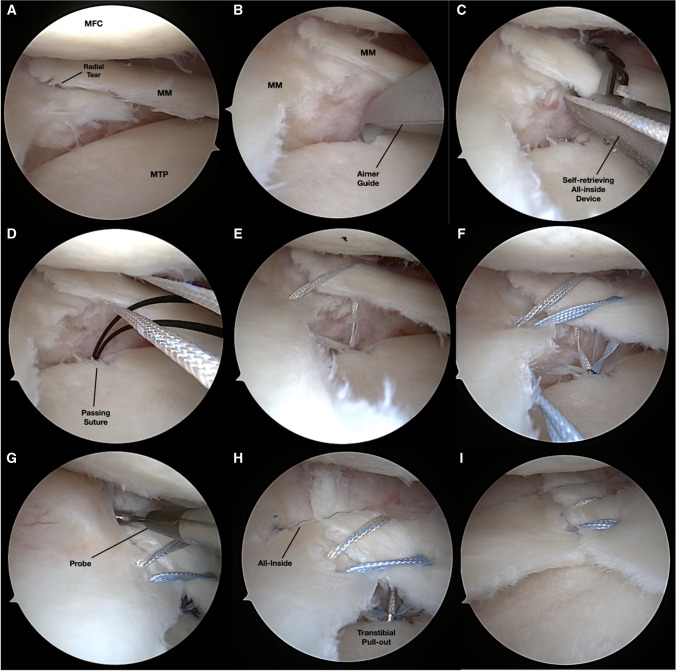
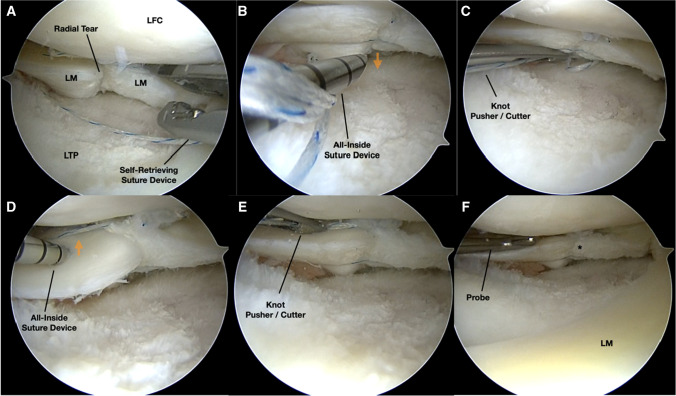
Recent findings: Recent literature shows that the repair of meniscus radial tears reports improved patient-reported outcome scores with high return to function and activity. However, no single technique nor construct was proven better than the other. Various methods of repairing radial tears can be employed, with biomechanical research supporting all-inside double vertical sutures, the addition of vertical "rip-stop" mattress sutures, and transtibial pullout augmentation. To ensure proper healing before undergoing physical therapy, it is crucial to abstain from weight-bearing and deep knee flexion for the first 6 weeks after surgery. Despite considerable heterogeneity in surgical techniques and rehabilitation protocols found in the current literature, studies reporting on radial repairs report positive results, with high healing rates and improved patient-reported outcomes.
Keywords: Meniscus radial tear; Meniscus repair; Postoperative outcomes.
© 2023. The Author(s), under exclusive licence to Springer Science+Business Media, LLC, part of Springer Nature.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Cullen KA, Hall MJ, Golosinskiy A. Ambulatory surgery in the United States, 2006. Natl Health Stat Report. 2009;11:1–25. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
