

Severely injured patients: modern management strategies
- PMID: 37158332
- PMCID: PMC10233811
- DOI: 10.1530/EOR-23-0053
Severely injured patients: modern management strategies
Abstract
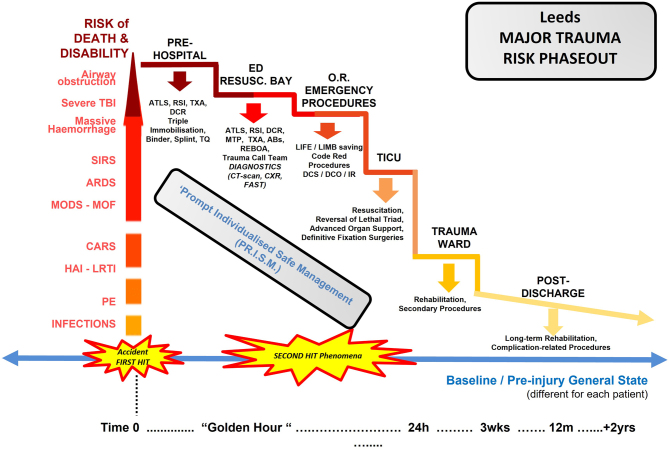
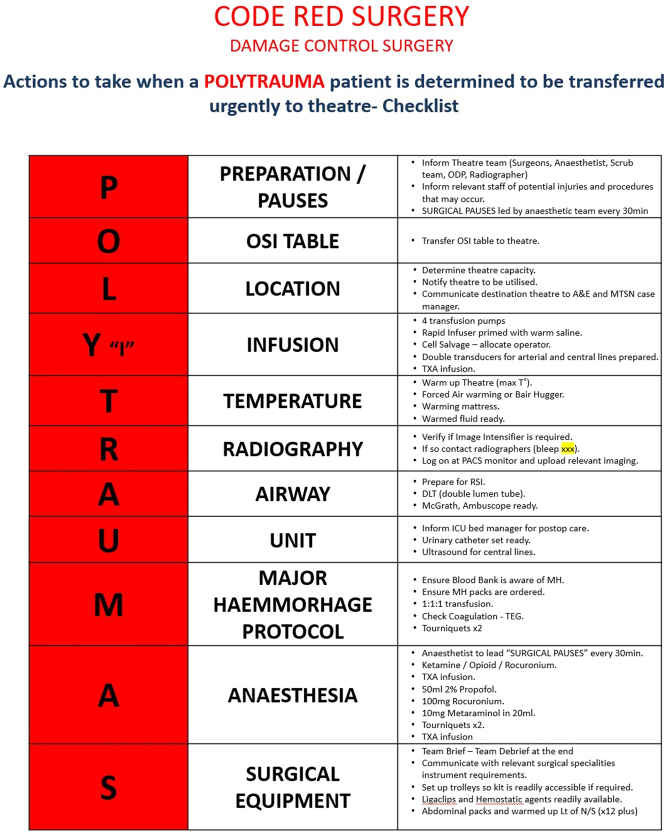
Management of severely injured patients remains a challenge, characterised by a number of advances in clinical practice over the last decades. This evolution refers to all different phases of patient treatment from prehospital to the long-term rehabilitation of the survivors. The spectrum of injuries and their severity is quite extensive, which dictates a clear understanding of the existing nomenclature. What is defined nowadays as polytrauma or major trauma, together with other essential terms used in the orthopaedic trauma literature, is described in this instructional review. Furthermore, an analysis of contemporary management strategies (early total care (ETG), damage control orthopaedics (DCO), early appropriate care (EAC), safe definitive surgery (SDS), prompt individualised safe management (PRISM) and musculoskeletal temporary surgery (MuST)) advocated over the last two decades is presented. A focused description of new methods and techniques that have been introduced in clinical practice recently in all different phases of trauma management will also be presented. As the understanding of trauma pathophysiology and subsequently the clinical practice continuously evolves, as the means of scientific interaction and exchange of knowledge improves dramatically, observing different standards between different healthcare systems and geographic regions remains problematic. Positive impact on the survivorship rates and decrease in disability can only be achieved with teamwork training on technical and non-technical skills, as well as with efficient use of the available resources.
Keywords: damage control; early appropriate care; major trauma; management; polytrauma; review.
Conflict of interest statement
All authors declare no conflict of interest.
Figures
References
-
- Wolrd Health Organisation. Injuries and violence. WHO; 2021. Available at: https://www.who.int/news-room/fact-sheets/detail/injuries-and-violence) (date last accessed 26 February 2023).
-
- Trauma Audit & Research Network, (TARN). Available at: https://www.tarn.ac.uk/ (date last accessed 26 February 2023).
-
- Association for the Advancement of Automotive Medicine 2019. Abbreviated Injury Scale (AIS) - overview. Available at: https://www.aaam.org/abbreviated-injury-scale-ais/ (date last accessed 26 February 2023).
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
