

Management of the stiff elbow: a literature review
- PMID: 37158372
- PMCID: PMC10233805
- DOI: 10.1530/EOR-23-0039
Management of the stiff elbow: a literature review
Abstract
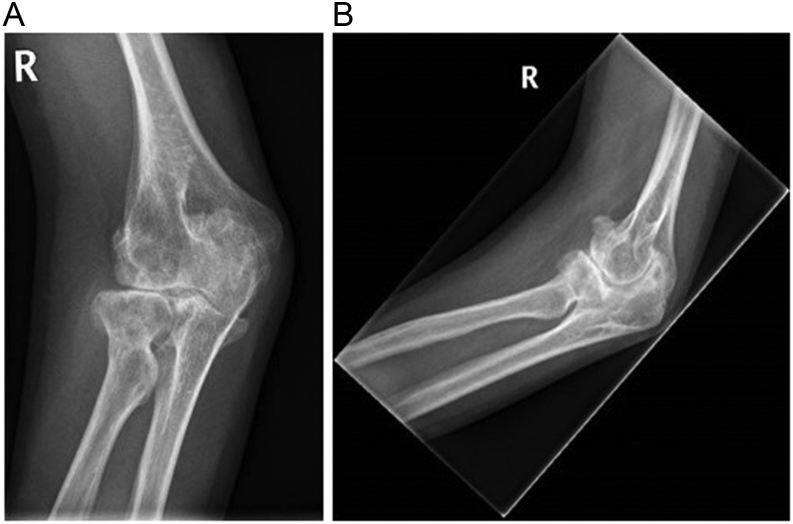
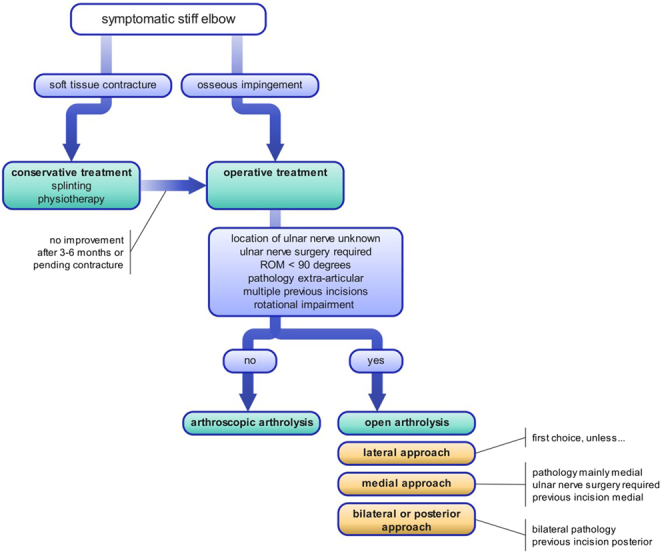
The elbow is prone to stiffness due to its unique anatomy and profound capsular reaction to inflammation. The resulting movement impairment may significantly interfere with a patient's activities of daily living. Trauma (including surgery for trauma), posttraumatic arthritis, and heterotopic ossification (HO) are the most common causes of elbow stiffness. In stiffness caused by soft tissue contractures, initial conservative treatment with physiotherapy (PT) and splinting is advised. In cases in which osseous deformities limit range of motion (e.g. malunion, osseous impingement, or HO), early surgical intervention is recommended. Open and arthroscopic arthrolysis are the primary surgical options. Arthroscopic arthrolysis has a lower complication and revision rate but has narrower indications. Early active mobilization using PT after surgery is recommended in postoperative rehabilitation and may be complemented by splinting or continuous passive motion therapy. Most results are gained within the first few months but can continue to improve until 12 months. This paper reviews the current literature and provides state-of-the-art guidance on the management regarding prevention, evaluation, and treatment of elbow stiffness.
Keywords: arthrofibrosis; osseous impingement; posttraumatic; soft tissue contracture; treatment.
Conflict of interest statement
The authors declare that there is no conflict of interest that could be perceived as prejudicing the impartiality of the research reported.
Figures





References
-
- O'Driscoll SW & Giori NJ. Continuous passive motion (CPM): theory and principles of clinical application. Journal of Rehabilitation Research and Development 200037179–188. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
