

Ziritaxestat, a Novel Autotaxin Inhibitor, and Lung Function in Idiopathic Pulmonary Fibrosis: The ISABELA 1 and 2 Randomized Clinical Trials
- PMID: 37159034
- PMCID: PMC10170340
- DOI: 10.1001/jama.2023.5355
Ziritaxestat, a Novel Autotaxin Inhibitor, and Lung Function in Idiopathic Pulmonary Fibrosis: The ISABELA 1 and 2 Randomized Clinical Trials
Abstract
Importance: There is a major need for effective, well-tolerated treatments for idiopathic pulmonary fibrosis (IPF).
Objective: To assess the efficacy and safety of the autotaxin inhibitor ziritaxestat in patients with IPF.
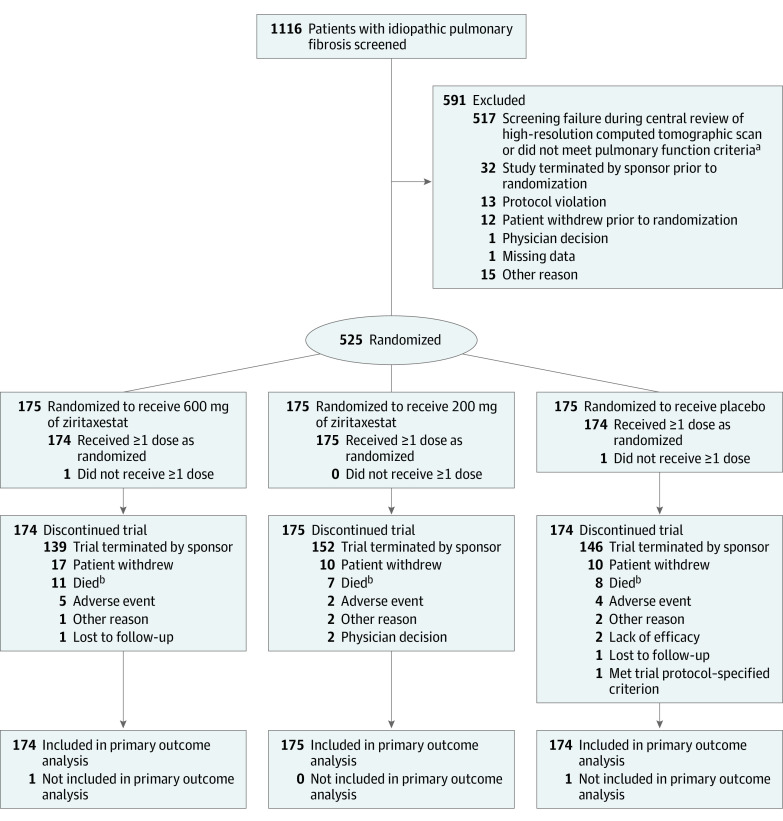
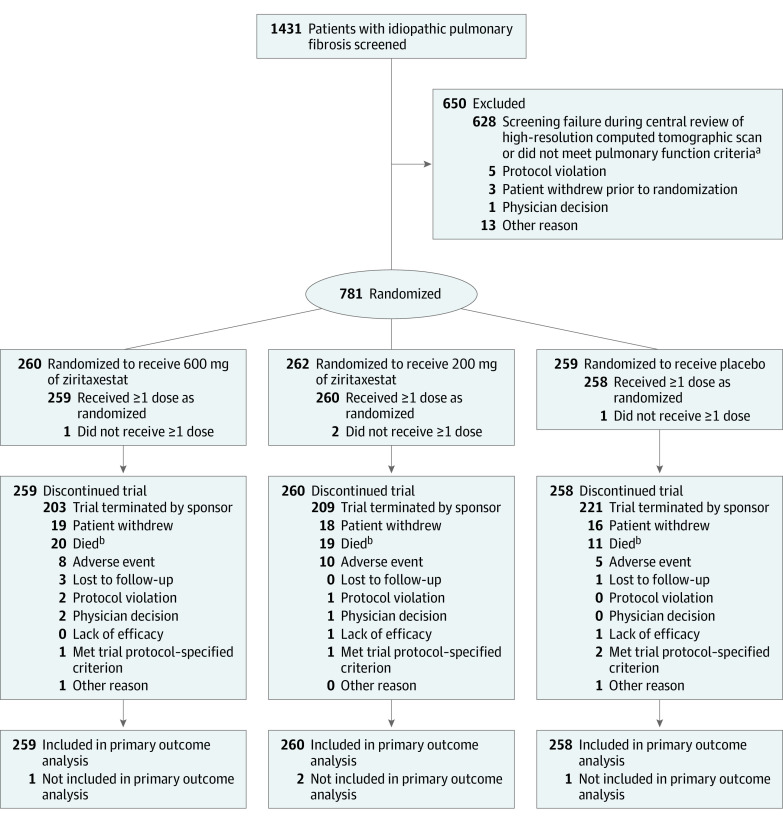
Design, setting, and participants: The 2 identically designed, phase 3, randomized clinical trials, ISABELA 1 and ISABELA 2, were conducted in Africa, Asia-Pacific region, Europe, Latin America, the Middle East, and North America (26 countries). A total of 1306 patients with IPF were randomized (525 patients at 106 sites in ISABELA 1 and 781 patients at 121 sites in ISABELA 2). Enrollment began in November 2018 in both trials and follow-up was completed early due to study termination on April 12, 2021, for ISABELA 1 and on March 30, 2021, for ISABELA 2.
Interventions: Patients were randomized 1:1:1 to receive 600 mg of oral ziritaxestat, 200 mg of ziritaxestat, or placebo once daily in addition to local standard of care (pirfenidone, nintedanib, or neither) for at least 52 weeks.
Main outcomes and measures: The primary outcome was the annual rate of decline for forced vital capacity (FVC) at week 52. The key secondary outcomes were disease progression, time to first respiratory-related hospitalization, and change from baseline in St George's Respiratory Questionnaire total score (range, 0 to 100; higher scores indicate poorer health-related quality of life).
Results: At the time of study termination, 525 patients were randomized in ISABELA 1 and 781 patients in ISABELA 2 (mean age: 70.0 [SD, 7.2] years in ISABELA 1 and 69.8 [SD, 7.1] years in ISABELA 2; male: 82.4% and 81.2%, respectively). The trials were terminated early after an independent data and safety monitoring committee concluded that the benefit to risk profile of ziritaxestat no longer supported their continuation. Ziritaxestat did not improve the annual rate of FVC decline vs placebo in either study. In ISABELA 1, the least-squares mean annual rate of FVC decline was -124.6 mL (95% CI, -178.0 to -71.2 mL) with 600 mg of ziritaxestat vs -147.3 mL (95% CI, -199.8 to -94.7 mL) with placebo (between-group difference, 22.7 mL [95% CI, -52.3 to 97.6 mL]), and -173.9 mL (95% CI, -225.7 to -122.2 mL) with 200 mg of ziritaxestat (between-group difference vs placebo, -26.7 mL [95% CI, -100.5 to 47.1 mL]). In ISABELA 2, the least-squares mean annual rate of FVC decline was -173.8 mL (95% CI, -209.2 to -138.4 mL) with 600 mg of ziritaxestat vs -176.6 mL (95% CI, -211.4 to -141.8 mL) with placebo (between-group difference, 2.8 mL [95% CI, -46.9 to 52.4 mL]) and -174.9 mL (95% CI, -209.5 to -140.2 mL) with 200 mg of ziritaxestat (between-group difference vs placebo, 1.7 mL [95% CI, -47.4 to 50.8 mL]). There was no benefit with ziritaxestat vs placebo for the key secondary outcomes. In ISABELA 1, all-cause mortality was 8.0% with 600 mg of ziritaxestat, 4.6% with 200 mg of ziritaxestat, and 6.3% with placebo; in ISABELA 2, it was 9.3% with 600 mg of ziritaxestat, 8.5% with 200 mg of ziritaxestat, and 4.7% with placebo.
Conclusions and relevance: Ziritaxestat did not improve clinical outcomes compared with placebo in patients with IPF receiving standard of care treatment with pirfenidone or nintedanib or in those not receiving standard of care treatment.
Trial registration: ClinicalTrials.gov Identifiers: NCT03711162 and NCT03733444.
Conflict of interest statement
Figures
Comment in
-
The Future of Clinical Trials in Idiopathic Pulmonary Fibrosis.JAMA. 2023 May 9;329(18):1554-1555. doi: 10.1001/jama.2022.23955. JAMA. 2023. PMID: 37159046 No abstract available.
-
Ziritaxestat and Lung Function in Idiopathic Pulmonary Fibrosis.JAMA. 2023 Sep 12;330(10):973. doi: 10.1001/jama.2023.12637. JAMA. 2023. PMID: 37698568 No abstract available.
References
-
- Martinez FJ, Collard HR, Pardo A, et al. Idiopathic pulmonary fibrosis. Nat Rev Dis Primers. 2017;3:17074. - PubMed
-
- Ley B, Collard HR, King TE Jr. Clinical course and prediction of survival in idiopathic pulmonary fibrosis. Am J Respir Crit Care Med. 2011;183(4):431-440. - PubMed
-
- Sharif R. Overview of idiopathic pulmonary fibrosis (IPF) and evidence-based guidelines. Am J Manag Care. 2017;23(11)(suppl):S176-S182. - PubMed
-
- Galli JA, Pandya A, Vega-Olivo M, et al. Pirfenidone and nintedanib for pulmonary fibrosis in clinical practice. Respirology. 2017;22(6):1171-1178. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
