

Colorectal neoplastic emergencies in immunocompromised patients: preliminary result from the Web-based International Register of Emergency Surgery and Trauma (WIRES-T trial)
- PMID: 37160552
- PMCID: PMC10435586
- DOI: 10.1007/s13304-023-01521-8
Colorectal neoplastic emergencies in immunocompromised patients: preliminary result from the Web-based International Register of Emergency Surgery and Trauma (WIRES-T trial)
Abstract
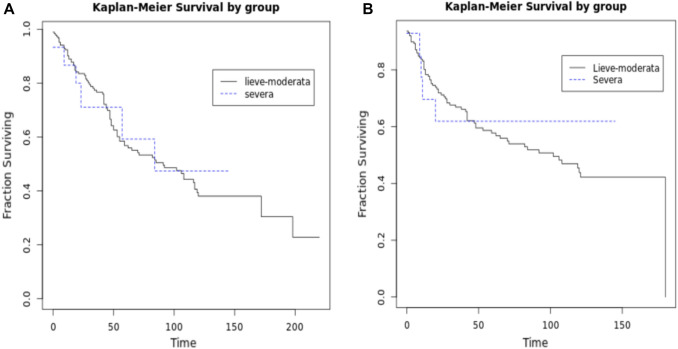
Association of advanced age, neoplastic disease and immunocompromission (IC) may lead to surgical emergencies. Few data exist about this topic. Present study reports the preliminary data from the WIRES-T trial about patients managed for colorectal neoplastic emergencies in immunocompromised patients. The required data were taken from a prospective observational international register. The study was approved by the Ethical Committee with approval n. 17575; ClinicalTrials.gov Identifier: NCT03643718. 839 patients were collected; 753 (80.7%) with mild-moderate IC and 86 (10.3%) with severe. Median age was 71.9 years and 73 years, respectively, in the two groups. The causes of mild-moderate IC were reported such malignancy (753-100%), diabetes (103-13.7%), malnutrition (26-3.5%) and uremia (1-0.1%), while severe IC causes were steroids treatment (14-16.3%); neutropenia (7-8.1%), malignancy on chemotherapy (71-82.6%). Preoperative risk classification were reported as follow: mild-moderate: ASA 1-14 (1.9%); ASA 2-202 (26.8%); ASA 3-341 (45.3%); ASA 4-84 (11.2%); ASA 5-7 (0.9%); severe group: ASA 1-1 patient (1.2%); ASA 2-16 patients (18.6%); ASA 3-41 patients (47.7%); ASA 4-19 patients (22.1%); ASA 5-3 patients (3.5%); lastly, ASA score was unavailable for 105 cases (13.9%) in mild-moderate group and in 6 cases (6.9%) in severe group. All the patients enrolled underwent urgent/emergency surgery Damage control approach with open abdomen was adopted in 18 patients. Mortality was 5.1% and 12.8%, respectively, in mild-moderate and severe groups. Long-term survival data: in mild-moderate disease-free survival (median, IQR) is 28 (10-91) and in severe IC, it is 21 (10-94). Overall survival (median, IQR) is 44 (18-99) and 26 (20-90) in mild-moderate and severe, respectively; the same is for post-progression survival (median, IQR) 29 (16-81) and 28, respectively. Univariate and multivariate analyses showed as the only factor influencing mortality in mild-moderate and severe IC is the ASA score. Colorectal neoplastic emergencies in immunocompromised patients are more frequent in elderly. Sigmoid and right colon are the most involved. Emergency surgery is at higher risk of complication and mortality; however, management in dedicated emergency surgery units is necessary to reduce disease burden and to optimize results by combining oncological and acute care principles. This approach may improve outcomes to obtain clinical advantages for patients like those observed in elective scenario. Lastly, damage control approach seems feasible and safe in selected patients.
Keywords: Acute care; Cancer; Colon; Emergency; Immunosuppression; Morbidity; Mortality; Surgery; Survival.
© 2023. The Author(s).
Conflict of interest statement
All the authors declare to have no conflict of interest.
Figures
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
