

Flash glucose monitoring in gestational diabetes mellitus (FLAMINGO): a randomised controlled trial
- PMID: 37160787
- PMCID: PMC10359198
- DOI: 10.1007/s00592-023-02091-2
Flash glucose monitoring in gestational diabetes mellitus (FLAMINGO): a randomised controlled trial
Erratum in
-
Correction: Flash glucose monitoring in gestational diabetes mellitus (FLAMINGO): a randomised controlled trial.Acta Diabetol. 2023 Oct;60(10):1439. doi: 10.1007/s00592-023-02159-z. Acta Diabetol. 2023. PMID: 37561211 Free PMC article. No abstract available.
Abstract
Aims: Gestational diabetes mellitus (GDM) is the most common type of hyperglycaemia in pregnancy. GDM is a risk factor of adverse perinatal outcomes, with the incidence rate increasing proportionally to the level of maternal dysglycaemia. Therefore, glycaemic control plays an important role in management of GDM. The aim of this study was to assess the efficacy of flash glucose monitoring (FGM) in GDM.
Materials and methods: This was a non-blinded, randomised controlled trial, that recruited 100 pregnant women diagnosed with GDM between 24 and 28 weeks of gestation at the 1st Department of Obstetrics and Gynaecology, Medical University of Warsaw. After meeting the inclusion criteria patients were randomly allocated to the study group (FGM, n = 50) or control group (self-monitoring of blood glucose-SMBG, n = 50). Clinical and laboratory results were assessed at four follow-up visits. The primary outcome was mean fasting and postprandial glycaemia. The secondary outcomes were perinatal outcomes.
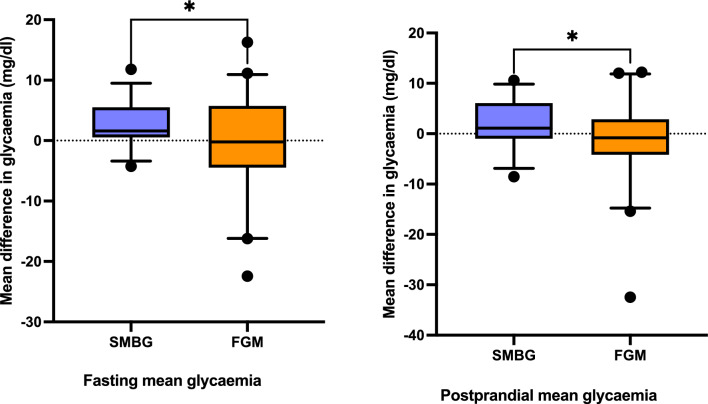
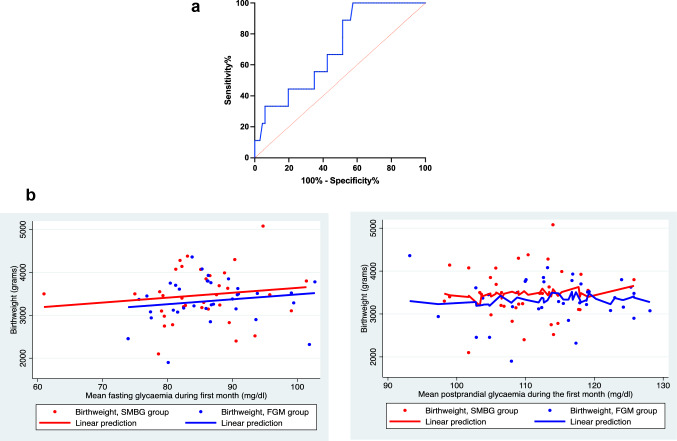
Results: There was no significant difference in mean glycaemia between the groups (p = 0.437) Compared to the control group, the study group significantly reduced their fasting (p = 0.027) and postprandial glycaemia (p = 0.034) during the first 4 weeks following GDM diagnosis, with no significant difference in progression to insulin therapy (OR 1.09, 95% CI 0.47-2.57). Incidence of fetal macrosomia was significantly higher in SMBG as compared to FGM group (OR 5.63, 95% CI 1.16-27.22).
Conclusions: Study results indicate that FGM has an impact on glycaemic control, dietary habits and incidence of fetal macrosomia in patients with GDM. Trial registration clinicaltrials.gov ID: NCT04422821.
Keywords: Dysglycaemia; Flash glucose monitoring; Gestational diabetes mellitus; Macrosomia.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Alberico S, Montico M, Barresi V, Monasta L, Businelli C, Soini V, et al. The role of gestational diabetes, pre-pregnancy body mass index and gestational weight gain on the risk of newborn macrosomia: results from a prospective multicentre study. BMC Pregnancy Childbirth. 2014;14:23. doi: 10.1186/1471-2393-14-23. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
