

Piperlongumine conquers temozolomide chemoradiotherapy resistance to achieve immune cure in refractory glioblastoma via boosting oxidative stress-inflamation-CD8+-T cell immunity
- PMID: 37161450
- PMCID: PMC10170830
- DOI: 10.1186/s13046-023-02686-1
Piperlongumine conquers temozolomide chemoradiotherapy resistance to achieve immune cure in refractory glioblastoma via boosting oxidative stress-inflamation-CD8+-T cell immunity
Abstract
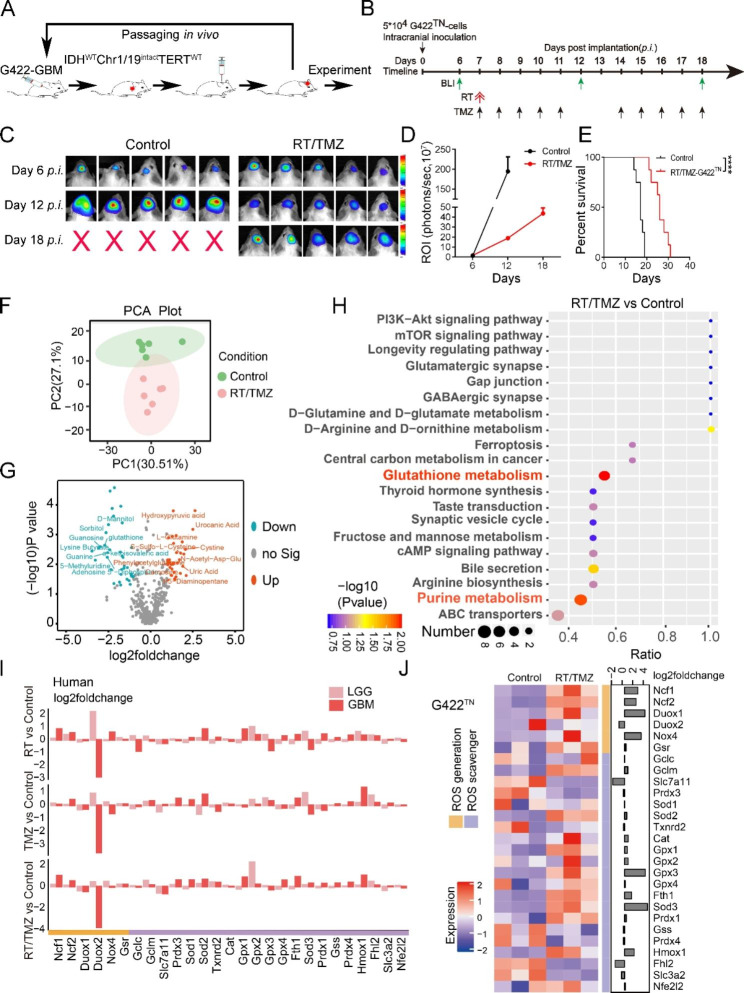
Background: The failure of novel therapies effective in preclinical animal models largely reflects the fact that current models do not really mimic the pathological/therapeutic features of glioblastoma (GBM), in which the most effective temozolomide chemoradiotherapy (RT/TMZ) regimen can only slightly extend survival. How to improve RT/TMZ efficacy remains a major challenge in clinic.
Methods: Syngeneic G422TN-GBM model mice were subject to RT/TMZ, surgery, piperlongumine (PL), αPD1, glutathione. Metabolomics or transcriptomics data from G422TN-GBM and human GBM were used for gene enrichment analysis and estimation of ROS generation/scavenging balance, oxidative stress damage, inflammation and immune cell infiltration. Overall survival, bioluminescent imaging, immunohistochemistry, and immunofluorescence staining were used to examine therapeutic efficacy and mechanisms of action.
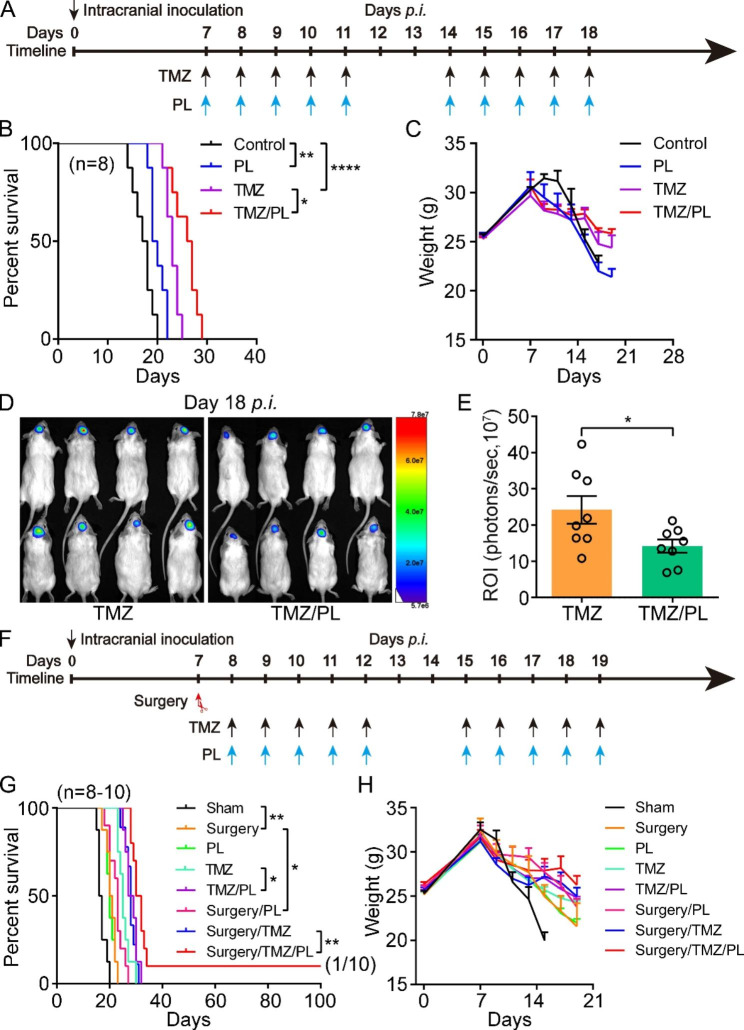
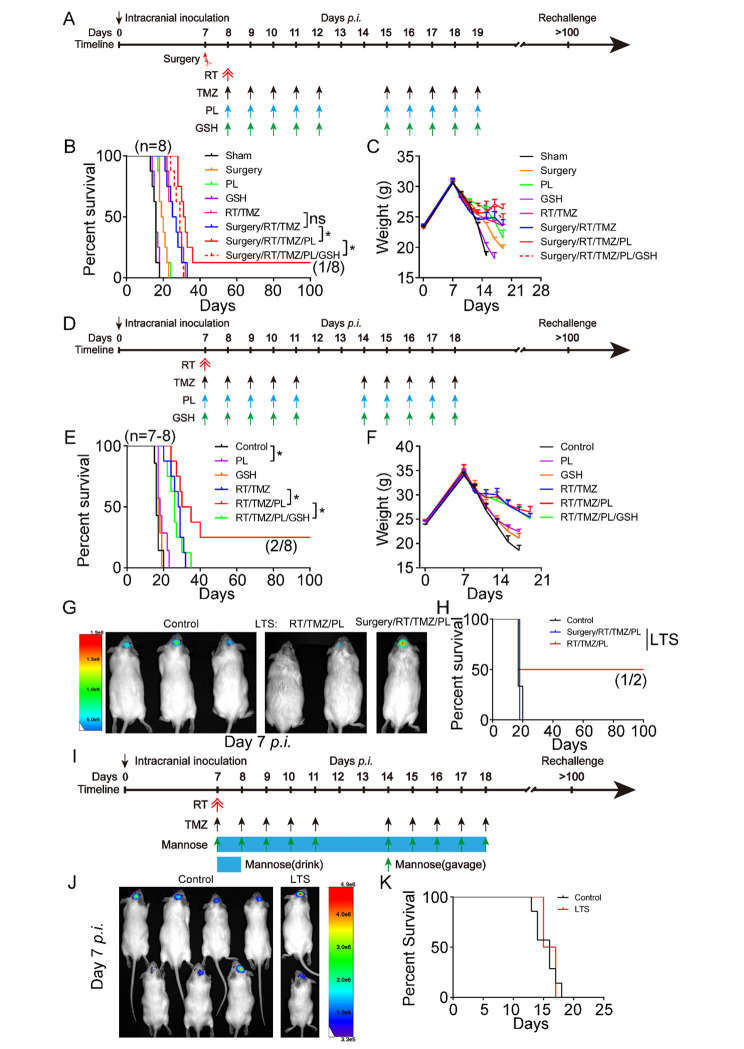
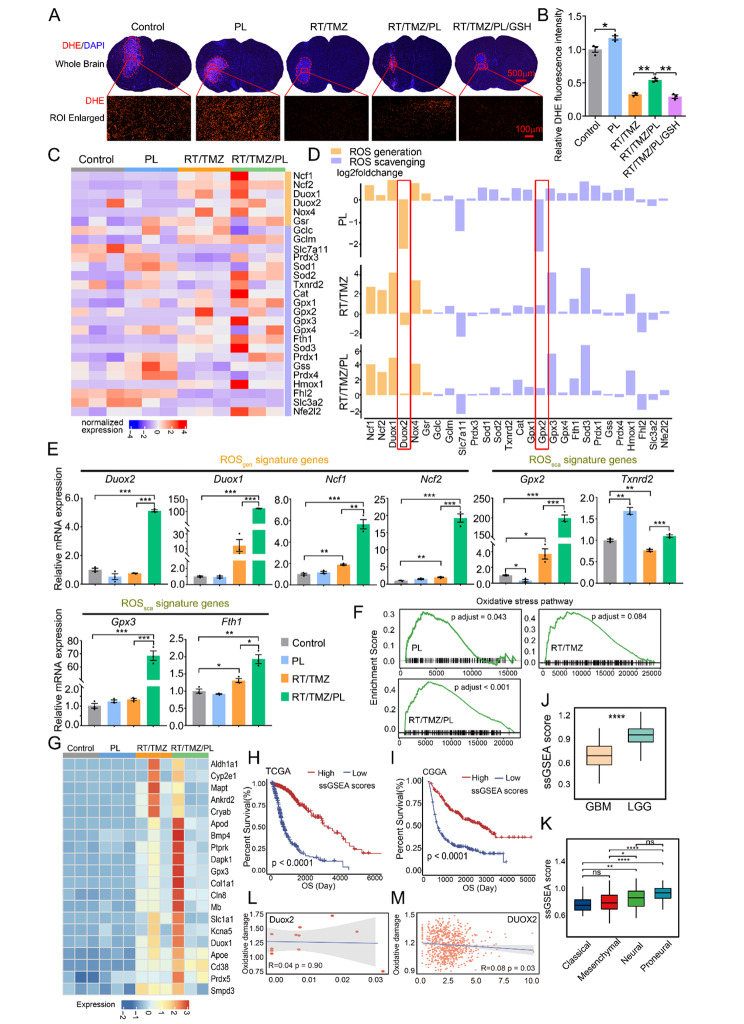
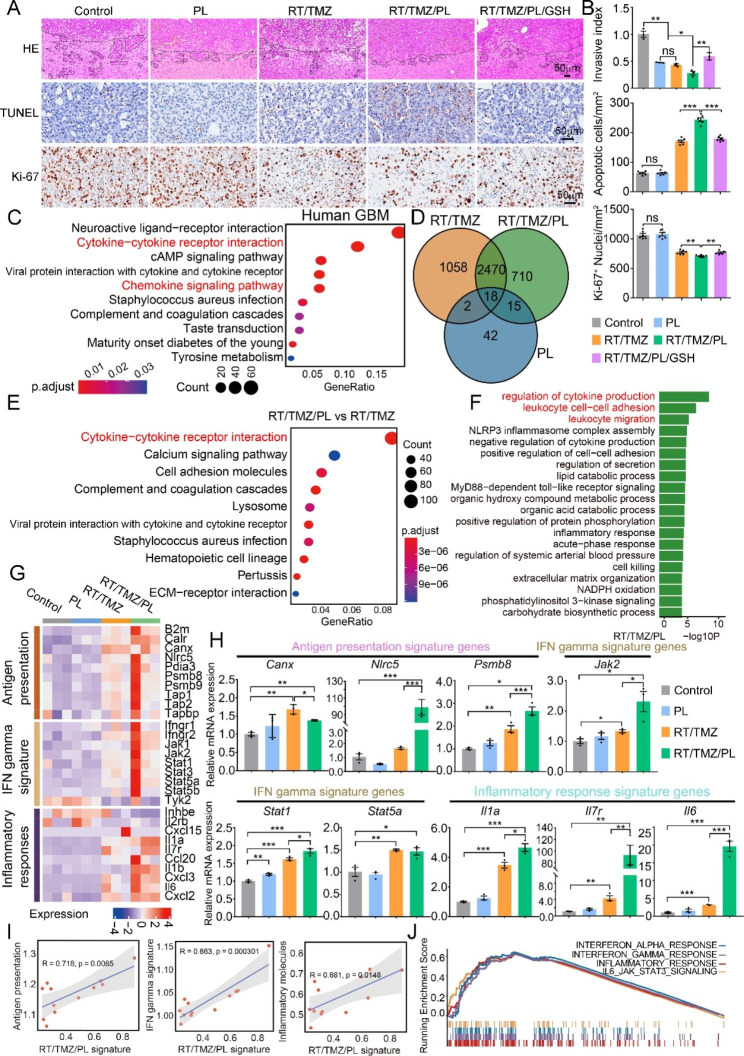
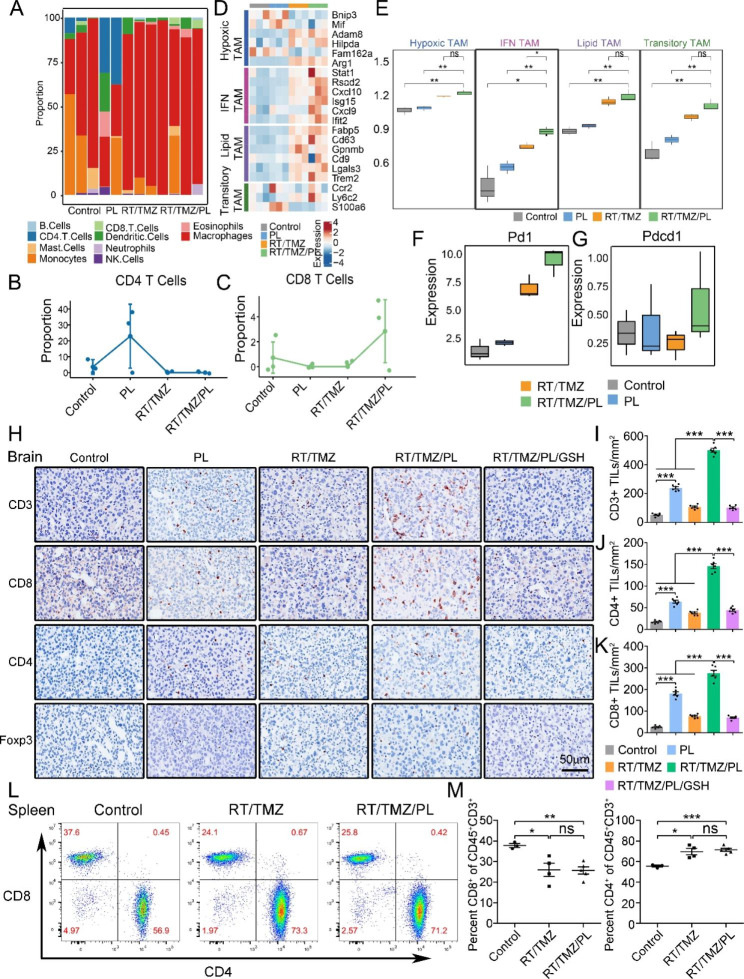
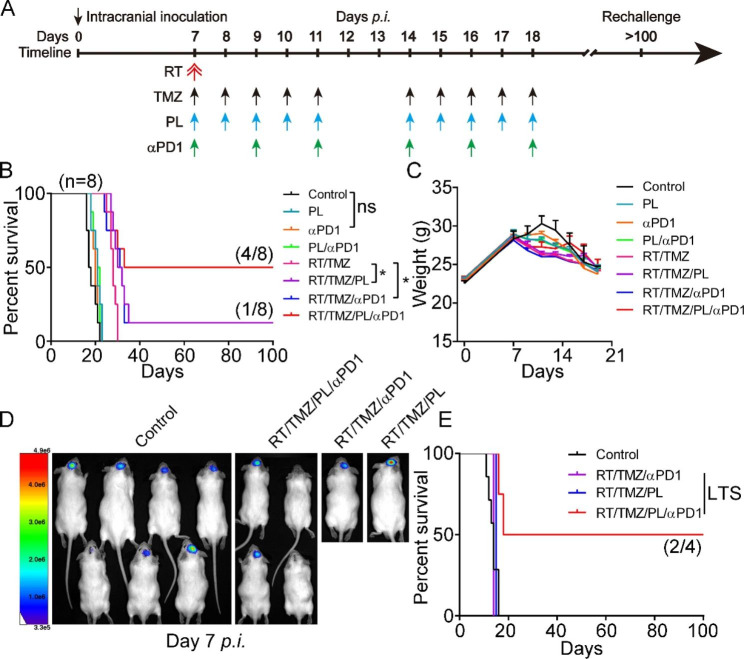
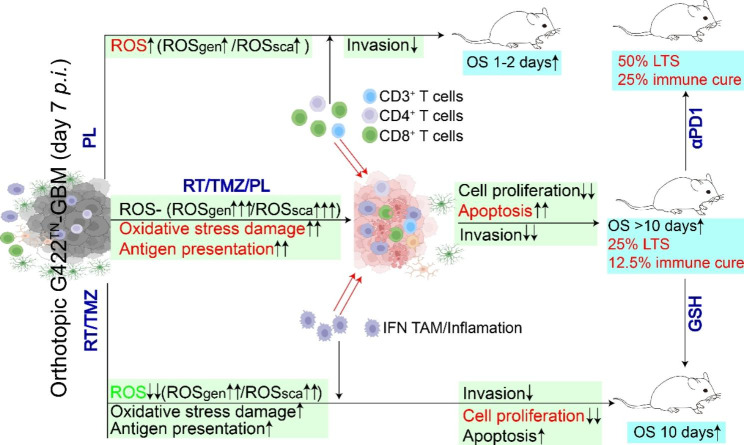
Results: Here we identified that glutathione metabolism was most significantly altered in metabolomics analysis upon RT/TMZ therapies in a truly refractory and reliable mouse triple-negative GBM (G422TN) preclinical model. Consistently, ROS generators/scavengers were highly dysregulated in both G422TN-tumor and human GBM. The ROS-inducer PL synergized surgery/TMZ, surgery/RT/TMZ or RT/TMZ to achieve long-term survival (LTS) in G422TN-mice, but only one LTS-mouse from RT/TMZ/PL therapy passed the rechallenging phase (immune cure). Furthermore, the immunotherapy of RT/TMZ/PL plus anti-PD-1 antibody (αPD1) doubled LTS (50%) and immune-cured (25%) mice. Glutathione completely abolished PL-synergistic effects. Mechanistically, ROS reduction was associated with RT/TMZ-resistance. PL restored ROS level (mainly via reversing Duox2/Gpx2), activated oxidative stress/inflammation/immune responses signature genes, reduced cancer cell proliferation/invasion, increased apoptosis and CD3+/CD4+/CD8+ T-lymphocytes in G422TN-tumor on the basis of RT/TMZ regimen.
Conclusion: Our findings demonstrate that PL reverses RT/TMZ-reduced ROS and synergistically resets tumor microenvironment to cure GBM. RT/TMZ/PL or RT/TMZ/PL/αPD1 exacts effective immune cure in refractory GBM, deserving a priority for clinical trials.
Keywords: Glioma; Immunotherapy; PD-1; Piperlongumine; ROS generation/elimination; Tumor microenvironment.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Stupp R, Hegi ME, Mason WP, van den Bent MJ, Taphoorn MJ, Janzer RC, et al. Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol. 2009;10(5):459–66. doi: 10.1016/S1470-2045(09)70025-7. - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials
