

Molnupiravir and risk of post-acute sequelae of covid-19: cohort study
- PMID: 37161995
- PMCID: PMC10126525
- DOI: 10.1136/bmj-2022-074572
Molnupiravir and risk of post-acute sequelae of covid-19: cohort study
Abstract
Objective: To examine whether treatment with the antiviral agent molnupiravir during the first five days of SARS-CoV-2 infection is associated with reduced risk of post-acute adverse health outcomes.
Design: Cohort study.
Setting: US Department of Veterans Affairs.
Participants: 229 286 participants who tested positive for SARS-CoV-2 between 5 January 2022 and 15 January 2023, had at least one risk factor for progression to severe covid-19, and survived the first 30 days after testing positive were enrolled. 11 472 participants received a prescription for molnupiravir within five days of the positive test result and 217 814 received no covid-19 antiviral or antibody treatment (no treatment group).
Main outcome measures: Risks of post-acute sequelae of SARS-CoV-2 (PASC, defined based on a prespecified set of 13 post-acute sequelae), post-acute death, post-acute hospital admission, and each individual post-acute sequela between the molnupiravir group and no treatment group were examined after application of inverse probability weighting to balance the treatment and no treatment groups. Post-acute outcomes were ascertained from 30 days after the first SARS-CoV-2 positive test result until end of follow-up. Risks on the relative scale (relative risk or hazard ratio) and absolute scale (absolute risk reduction at 180 days) were estimated.
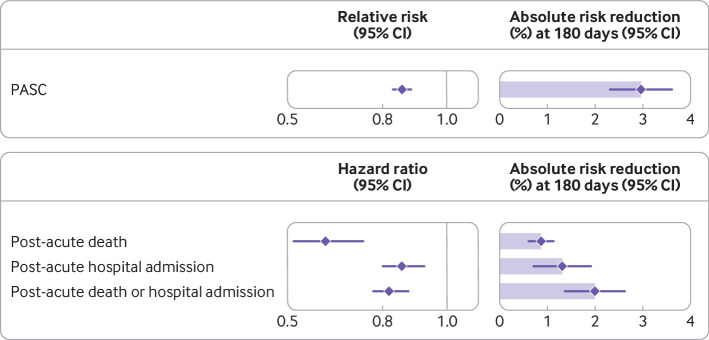
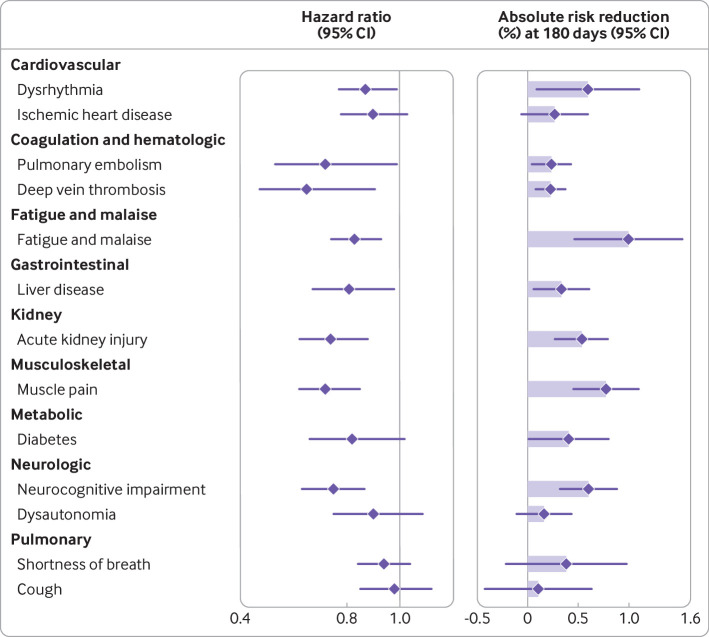
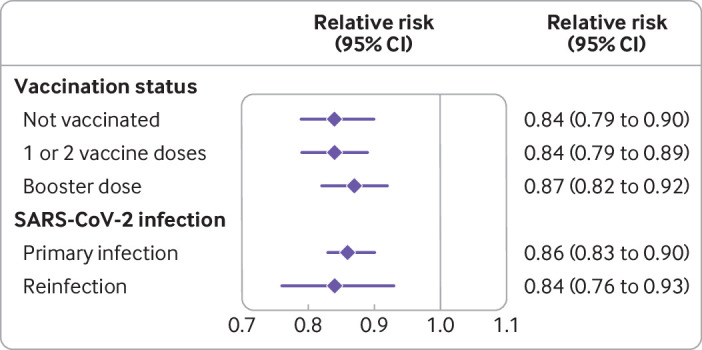
Results: Compared with no treatment, molnupiravir use within five days of a positive SARS-CoV-2 test result was associated with reduced risk of PASC (relative risk 0.86 (95% confidence interval 0.83 to 0.89); absolute risk reduction at 180 days 2.97% (95% confidence interval 2.31% to 3.60%)), post-acute death (hazard ratio 0.62 (0.52 to 0.74); 0.87% (0.62% to 1.13%)), and post-acute hospital admission (0.86 (0.80 to 0.93); 1.32% (0.72% to 1.92%)). Molnupiravir was associated with reduced risk of eight of the 13 post-acute sequelae: dysrhythmia, pulmonary embolism, deep vein thrombosis, fatigue and malaise, liver disease, acute kidney injury, muscle pain, and neurocognitive impairment. Molnupiravir was also associated with reduced risk of PASC in people who had not received a covid-19 vaccine, had received at one or two vaccine doses, and had received a booster dose, and in people with primary SARS-CoV-2 infection and reinfection.
Conclusions: In people with SARS-CoV-2 infection and at least one risk factor for progression to severe covid-19, compared with no treatment, molnupiravir use within five days of infection was associated with reduced risk of PASC in people who had not received a covid-19 vaccine, had received one or two vaccine doses, and had received a booster dose, and in those with primary SARS-CoV-2 infection and reinfection. Among people at high risk of progression to severe covid-19, molnupiravir use within five days of SARS-CoV-2 infection may be a viable approach to reduce the risk of PASC.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: support from the US Department of Veterans Affairs for the submitted work. ZAA reports receiving consultation fees from Gilead Sciences and receipt of funding (unrelated to this work) from Tonix pharmaceuticals. ZAA and YX reports consulting (uncompensated) for Pfizer; no other relationships or activities that could appear to have influenced the submitted work.
Figures


References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous