

Tropifexor plus cenicriviroc combination versus monotherapy in nonalcoholic steatohepatitis: Results from the phase 2b TANDEM study
- PMID: 37162151
- PMCID: PMC10521801
- DOI: 10.1097/HEP.0000000000000439
Tropifexor plus cenicriviroc combination versus monotherapy in nonalcoholic steatohepatitis: Results from the phase 2b TANDEM study
Abstract
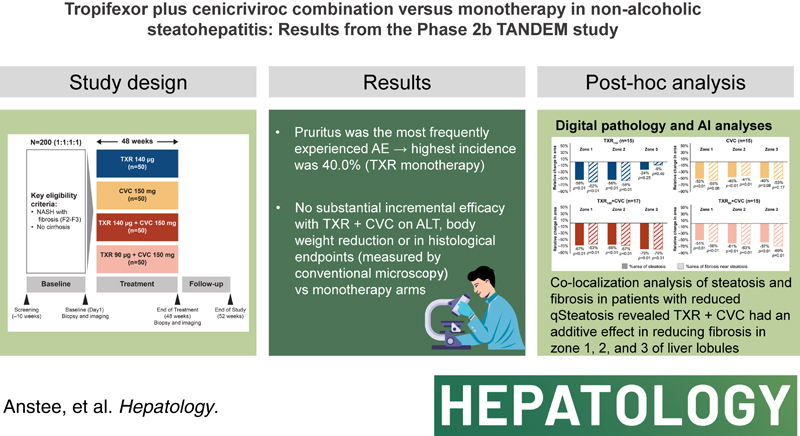
Background and aims: With distinct mechanisms of action, the combination of tropifexor (TXR) and cenicriviroc (CVC) may provide an effective treatment for NASH. This randomized, multicenter, double-blind, phase 2b study assessed the safety and efficacy of TXR and CVC combination, compared with respective monotherapies.
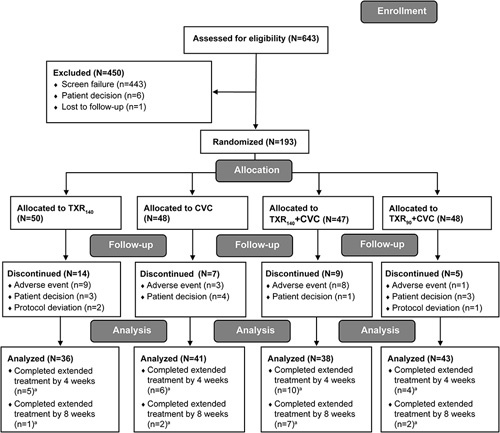
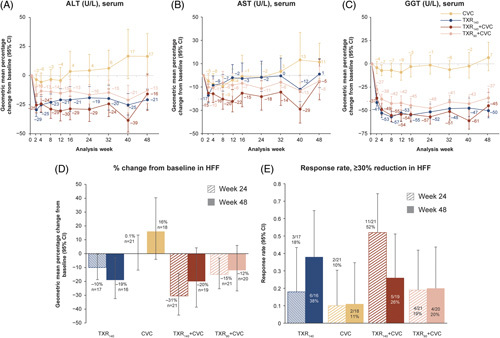
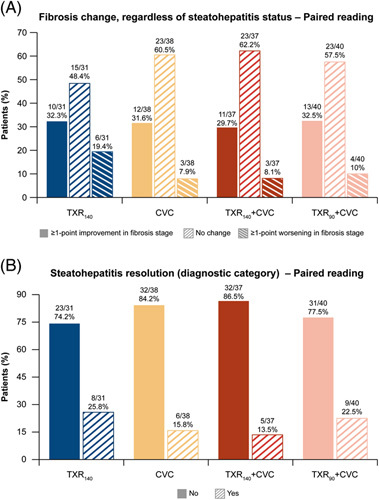
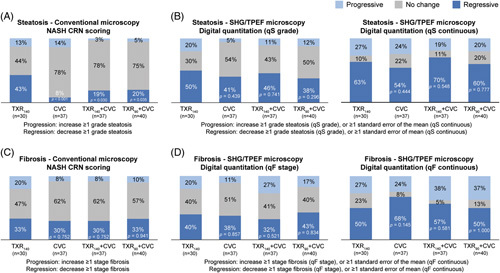
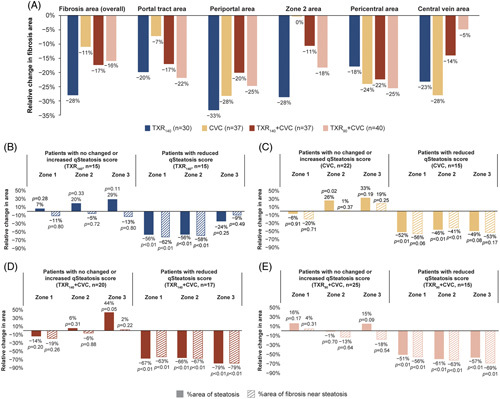
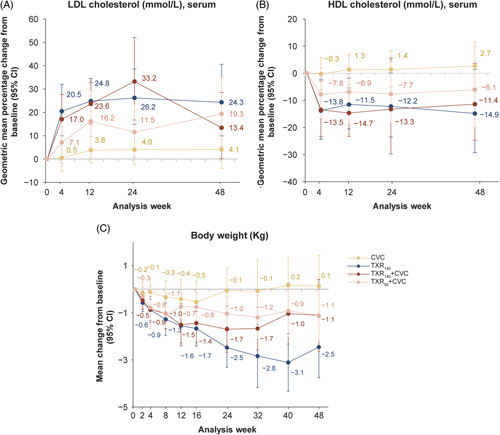
Approach and results: Patients (N = 193) were randomized 1:1:1:1 to once-daily TXR 140 μg (TXR 140 ), CVC 150 mg (CVC), TXR 140 μg + CVC 150 mg (TXR 140 + CVC), or TXR 90 μg + CVC 150 mg (TXR 90 + CVC) for 48 weeks. The primary and secondary end points were safety and histological improvement, respectively. Rates of adverse events (AEs) were similar across treatment groups. Pruritus was the most frequently experienced AE, with highest incidence in the TXR 140 group (40.0%). In TXR and combination groups, alanine aminotransferase (ALT) decreased from baseline to 48 weeks (geometric mean change: -21%, TXR 140 ; -16%, TXR 140 + CVC; -13%, TXR 90 + CVC; and +17%, CVC). Reductions in body weight observed at week 24 (mean changes from baseline: TXR 140 , -2.5 kg; TXR 140 + CVC, -1.7 kg; TXR 90 + CVC, -1.0 kg; and CVC, -0.1 kg) were sustained to week 48. At least 1-point improvement in fibrosis stage/steatohepatitis resolution without worsening of fibrosis was observed in 32.3%/25.8%, 31.6%/15.8%, 29.7%/13.5%, and 32.5%/22.5% of patients in the TXR 140 , CVC, TXR 140 + CVC, and TXR 90 + CVC groups, respectively.
Conclusions: The safety profile of TXR + CVC combination was similar to respective monotherapies, with no new signals. TXR monotherapy showed sustained ALT and body weight decreases. No substantial incremental efficacy was observed with TXR + CVC combination on ALT, body weight, or in histological end points compared with monotherapy.
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
Quentin M. Anstee, on behalf of Newcastle University, consults for Alimentiv, Akero, AstraZeneca, Axcella, 89 Bio, Boehringer Ingelheim, Bristol Myers Squibb, Galmed, Genfit, Genentech, Gilead, GlaxoSmithKline, Hanmi, HistoIndex, Intercept, Inventiva, Ionis, IQVIA, Janssen, Madrigal, Medpace, Merck, NGM Bio, Novartis, Novo Nordisk, PathAI, Pfizer, Pharmanest, Prosciento, Poxel, Resolution Therapeutics, Roche, Ridgeline Therapeutics, RTI, Shionogi, and Terns. He received grants from AstraZeneca, Boehringer Ingelheim, and Intercept. He is on the speakers’ bureau for Fishawack, Integritas Communications, Kenes, Novo Nordisk, Madrigal, Medscape, and Springer Healthcare. He receives royalties from Elsevier. He is Coordinator of the EU-IMI-2 LITMUS consortium, which is funded by the EU Horizon 2020 programme and EFPIA. Sven Francque consults for, is on the speakers’ bureau for, and received grants from Genfit, Gilead, Janssen, Inventiva, and MSD. He consults for and is on the speakers’ bureau for Abbvie, Allergan, Bayer, Eisai, Intercept, Novo Nordisk, and Promethera. He consults for and received grants from Astellas and Roche. He consults for Actelion, Aelin Therapeutics, AgomAb, Aligos Therapeutics, AstraZeneca, BMS, Boheringer Ingelheim, CSL Behring, Coherus, Echosens, Enyo, Galapagos, Galmed, Genentech, Intercept, Julius Clinical, Madrigal, Medimmune, NGM Bio, and Novartis. He received grants from Falk Pharma, GlympseBio, and Pfizer. He holds a senior clinical investigator fellowship from the Research Foundation Flanders (FWO) (1802154N). Manal F. Abdelmalek consults for, advises, and received grants from Hanmi, Inventiva, and Novo Nordisk. She advises and received grants from Madrigal, BMS, and NGM Bio. She advises SonicIncytes, 89 Bio, Merck, and Theratechnologies. She is on the speakers’ bureau for Clinical Care Options, Fishawack, Medscape, Terra Firma, and CLDF. She received grants from Allergan, Boeringher-Ingelheim, Celegene, Durect, Enanta, Enyo, Galmed, Genetech, Gilead, Poxel, Target NASH, and Viking. Her institution received grants from 89 Bio, Enyo, Enanta, Durect, Celegene, Poxel, Genfit, Gilead, Genentech, Novartis, Novo Nordisk, Hanmi, Inventiva, BMS, Boehringer Ingelheim, Intercept, and Novo Nordisk. Arun J. Sanyal owns stock and consults for Genfit and Hemoshear. He consults for and received grants from Boehringer Ingelheim, Lilly, Novo Nordisk, Fractyl, Siemens, Madrigal, Inventiva, and Echosense-Sandhill. He consults for Intercept, Immuron, Pfizer, Salix, Sanofi, Sequana, Terns, Albireo, Jannsen, Poxel, 89 Bio, Astrazeneca, NGM Bio, Amgen, Afimmune, Bristol Myers Squibb, Regeneron, Gilead Galectin, Genentech, Glympse, Birdrock, Blade, Target-Pharma Teva, Artham, Salix, Alnylam, Roche, Chemomab, Covance, Conatus, Cumberland, Merck, Prosciento, Syntolgic, Surrozen, Histoindex, Malinckrodt, Nitto Denko, Nordic Biosciences, Novartis, Nimbus, Tobira, Valeant, Zafgen, Zydus, and Path AI. He owns stock in and consults for Exhalez, Galmed, and Takeda. He received grants from Second Genome, Cymabay, and Labcorp. He owns stock in Akarna, Durect, Indalo, Inversago, NorthSea, Tiziana, and Rivus. His institution has received grants from Gilead, Salix, Tobira, Bristol Myers, Shire, Intercept, Merck, AstraZeneca, Malinckrodt, Cumberland, and Novartis. He receives royalties from Up-To-Date and Elsevier. He is president of Sanyal Bio. Vlad Ratziu consults and received grants from Intercept. He consults for Boehringer Ingelheim, Novo Nordisk, Sagimet, Terns, NGM Bio, Pfizer, North Sea, Madrigal, Enyo, and Poxel. He received grants from Gilead. Adrian C. Gadano is a national coordinator for Novo Nordisk. He is a principal investigator for BMS, Novo Nordisk, GSK. Michael Charlton consults for, advises, and received grants from Gilead. He consults for and received grants from Novartis. He consults for AbbVie, Intercept, Terns, Madrigal, Metacrine, Enterome, Sagmiet, North Sea, NGM Bio, Pfizer, and Merck. He received grants from Novartis, Conatus, and Galectin. Rohit Loomba consults for Aardvark Therapeutics, Altimmune, Anylam/Regeneron, Amgen, Arrowhead Pharmaceuticals, AstraZeneca, Bristol-Myer Squibb, CohBar, Eli Lilly, Galmed, Gilead, Glympse Bio, Hightide, Inipharma, Intercept, Inventiva, Ionis, Janssen Inc., Madrigal, Metacrine, Inc., NGM Biopharmaceuticals, Novartis, Novo Nordisk, Merck, Pfizer, Sagimet, Theratechnologies, 89 bio, Terns Pharmaceuticals, and Viking Therapeutics. His institution received research grants from Arrowhead Pharmaceuticals, Astrazeneca, Boehringer Ingelheim, Bristol Myers Squibb, Eli Lilly, Galectin Therapeutics, Galmed Pharmaceuticals, Gilead, Hanmi, Intercept, Inventiva, Ionis, Janssen, Madrigal Pharmaceuticals, Merck, NGM Biopharmaceuticals, Novo Nordisk, Pfizer, Sonic Incytes, and Terns Pharmaceuticals. He is the co-founder of LipoNexus Inc. Edward Mena consults for and is on the speakers’ bureau for Gilead, AbbVie, Eisai, and Salix. He is on the speakers’ bureau for Intercept. Jörn M. Schattenberg consults for, is on the speakers’ bureau for, and received grants from Boehringer Ingelheim. He consults for and is on the speakers’ bureau for Novo Nordisk and Madrigal. He consults for and received grants from Gilead Sciences and Siemens Healthcare GmbH. He consults for Apollo Endosurgery, Albireo, BMS, AGED diagnostics, Bayer, GSK, Intercept Pharmaceuticals, Ipsen, Inventiva Pharma, MSD, Northsea Therapeutics, Novartis, Pfizer, Roche, and Sanofi. He is on the speakers’ bureau for Echosens, MedPublico GmbH, and Histoindex. He received grants from Nordic Biosciences. Mazen Noureddin consults for, advises, and received grants from BMS, Gilead, Novo Nordisk, and Terns. He consults for and advises Altimmune, Boehringer Ingelheim, 89 Bio, Echosens, GSK, Merck, OWL, Pfizer, Roche, Siemens, and Takeda. He received grants from Allergan, Akero, Galectin, Genfit, Conatus, Corcept, Enanta, Madrigal, Novartis, Shire, Viking, and Zydus. He owns stock in Anaetos, Rivus Pharma, CIMA, ChronWell, and Viking. George B.B. Goh consults for Gilead, Boehringer Ingelheim, and Ionis Pharmaceuticals. He is on the speakers’ bureau for Novo Nordisk and Echosens. Yusuf Yilmaz consults for Zydus and Novo Nordisk. He is on the speakers’ bureau for Echosens. Miljen Martic is employed by and owns stock in Novartis. Rowan Stringer is employed by and owns stock in Novartis. Jossy Kochuparampil owns stock in and is employed by Novartis. Li Chen owns stock in and is employed by Novartis. Gerardo Rodriguez-Araujo owns stock in and is employed by AbbVie. Elaine Chng is employed by Histoindex. Nikolai V. Naoumov owns stock in and was employed by Novartis. He advises Histoindex. Clifford Brass owns stock in, was employed by, and owns intellectual property rights with Novartis. He owns stock in Merck. He is a Scientific Advisory Board member of EU-IMI 2 LITMUS consortium. Marcos C. Pedrosa owns stock, was employed by, and consults for Novartis. The remaining authors have no conflicts to report.
Figures
References
-
- Younossi ZM, Koenig AB, Abdelatif D, Fazel Y, Henry L, Wymer M. Global epidemiology of nonalcoholic fatty liver disease-meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology. 2016;64:73–84. - PubMed
-
- Diehl AM, Day C. Cause, pathogenesis, and treatment of nonalcoholic steatohepatitis. N Engl J Med . 2017;377:2063–72. - PubMed
-
- Moschen AR, Kaser S, Tilg H. Non-alcoholic steatohepatitis: A microbiota-driven disease. Trends Endocrinol Metab. 2013;24:537–45. - PubMed
