

Catastrophic ACTH-secreting pheochromocytoma: an uncommon and challenging entity with multifaceted presentation
- PMID: 37162230
- PMCID: PMC10266445
- DOI: 10.1530/EDM-22-0308
Catastrophic ACTH-secreting pheochromocytoma: an uncommon and challenging entity with multifaceted presentation
Abstract
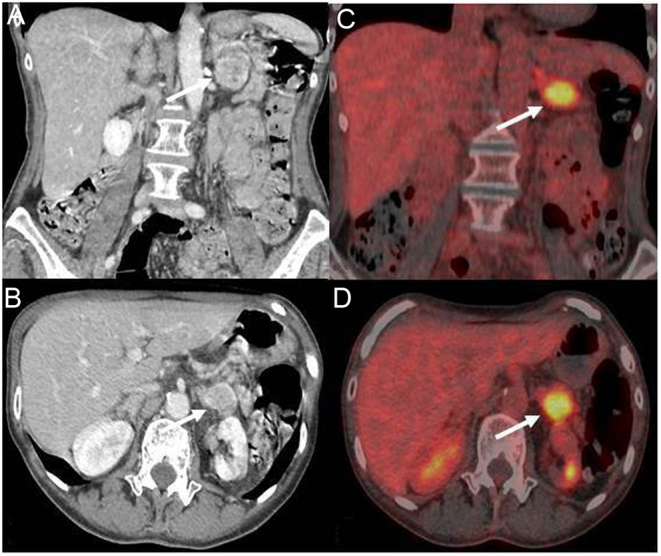
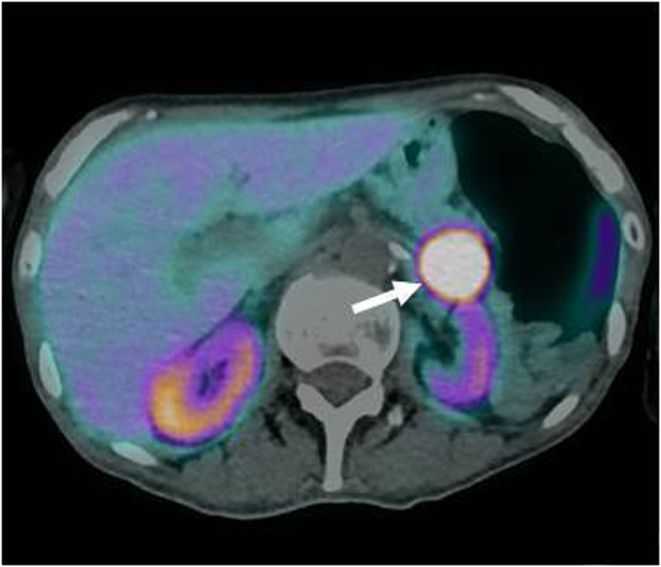
Summary: Cushing's syndrome due to ectopic adrenocorticotropic hormone (ACTH) secretion (EAS) by a pheochromocytoma is a challenging condition. A woman with hypertension and an anamnestic report of a 'non-secreting' left adrenal mass developed uncontrolled blood pressure (BP), hyperglycaemia and severe hypokalaemia. ACTH-dependent severe hypercortisolism was ascertained in the absence of Cushingoid features, and a psycho-organic syndrome developed. Brain imaging revealed a splenial lesion of the corpus callosum and a pituitary microadenoma. The adrenal mass displayed high uptake on both 18F-FDG PET/CT and 68Ga-DOTATOC PET/CT; urinary metanephrine levels were greatly increased. The combination of antihypertensive drugs, high-dose potassium infusion, insulin and steroidogenesis inhibitor normalized BP, metabolic parameters and cortisol levels; laparoscopic left adrenalectomy under intravenous hydrocortisone infusion was performed. On combined histology and immunohistochemistry, an ACTH-secreting pheochromocytoma was diagnosed. The patient's clinical condition improved and remission of both hypercortisolism and catecholamine hypersecretion ensued. Brain magnetic resonance imaging showed a reduction of the splenial lesion. Off-therapy BP and metabolic parameters remained normal. The patient was discharged on cortisone replacement therapy for post-surgical hypocortisolism. EAS due to pheochromocytoma displays multifaceted clinical features and requires prompt diagnosis and multidisciplinary management in order to overcome the related severe clinical derangements.
Learning points: A small but significant number of cases of adrenocorticotropic hormone (ACTH)-dependent Cushing's syndrome are caused by ectopic ACTH secretion by neuroendocrine tumours, which is usually associated with severe hypercortisolism causing severe clinical and metabolic derangements. Ectopic ACTH secretion by a pheochromocytoma is exceedingly rare but can be life-threatening, owing to the simultaneous excess of both cortisol and catecholamines. The combination of biochemical and hormonal testing and imaging procedures is mandatory for the diagnosis of ectopic ACTH secretion, and in the presence of an adrenal mass, the possibility of an ACTH-secreting pheochromocytoma should be taken into account. Immediate-acting steroidogenesis inhibitors are required for the treatment of hypercortisolism, and catecholamine excess should also be appropriately managed before surgical removal of the tumour. A multidisciplinary approach is required for the treatment of this challenging entity.
Conflict of interest statement
The authors declare that there is no conflict of interest that could be perceived as prejudicing the impartiality of the research reported.
Figures



References
-
- Fleseriu M, Auchus R, Bancos I, Ben-Shlomo A, Bertherat J, Biermasz NR, Boguszewski CL, Bronstein MD, Buchfelder M, Carmichael JD, et al. Consensus on diagnosis and management of Cushing's disease: a guideline update. Lancet. Diabetes and Endocrinology 20219847–875. ( 10.1016/S2213-8587(2100235-7) - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
